Volume 1, Issue 2, Literature Review Article – Dec 29, 2025, Pages 52-60
DOI: 10.64951/jmdnt.2026.1.06
Mandibular Reconstruction with Fibula Flap and Dental Implants Through Virtual Surgical Planning: A Systematic Review of Three Techniques – Double-Barrel Flap, CAD/CAM Titanium Mesh with Iliac Crest Graft, and Intraoperative Dynamic Implant Navigation
Ayhan Yildirim¹, René Hertach², Vedat Yildirim²
¹ Hochschule Zurich, Department of Medicine, Albisstrasse 80, 8038 Zurich, Switzerland
² Hochschule Zurich, Department of Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland
Received: 08 June 2025, Revised: 21 October 2025, Accepted: 16 November 2025, Available online: 07 December 2025, Version of Record: 29 December 2025
© 2025 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
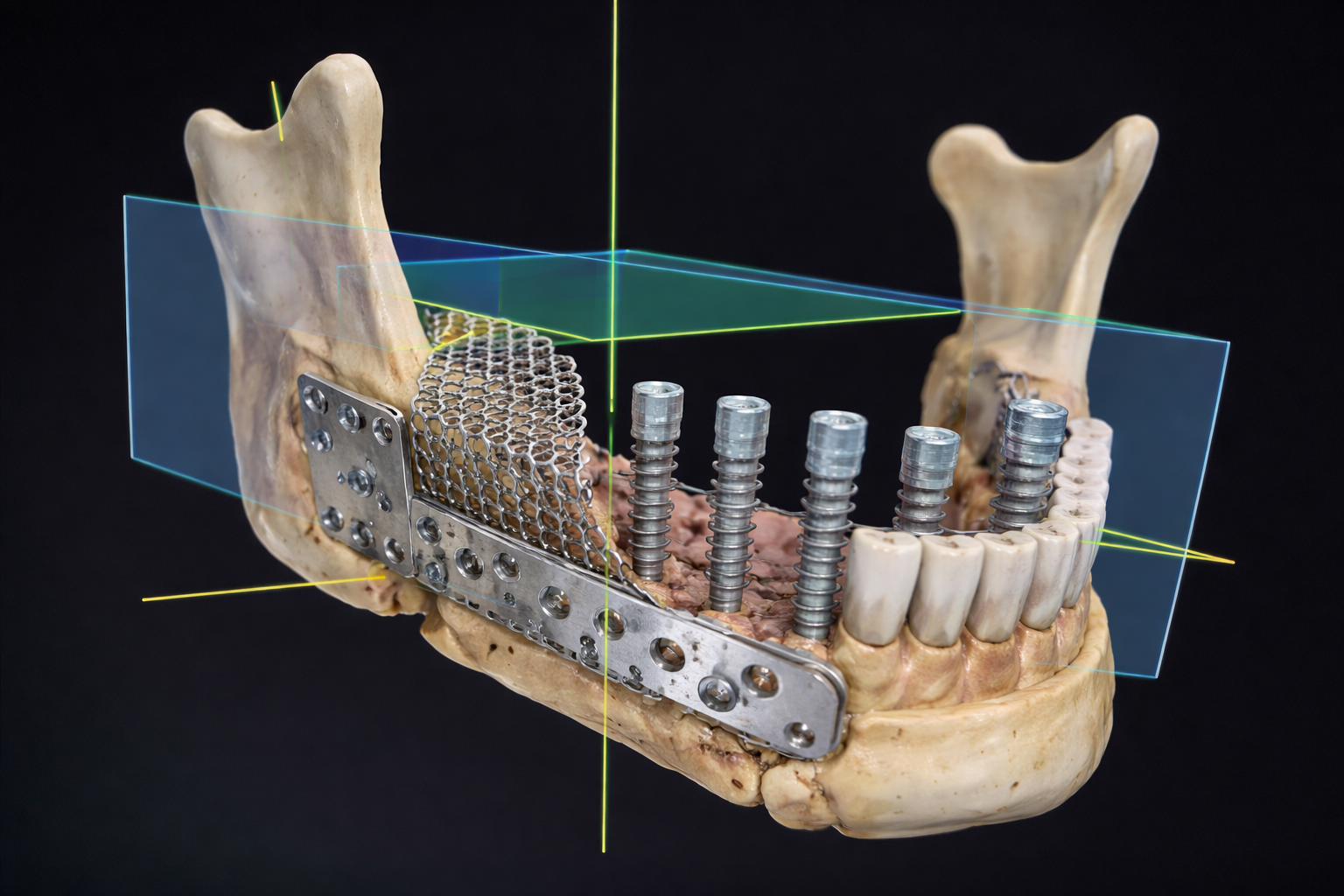
Three-dimensional virtual surgical planning (VSP) screenshot illustrating the reconstructed mandible. The color-coded mandibular model demonstrates precise spatial alignment of the fibula free flap segments, customized titanium fixation hardware, and planned dental implant positions. The visualization highlights vertical bone reconstruction, implant trajectory, and prosthetically driven alignment achieved through computer-assisted planning, serving as the basis for CAD/CAM-guided osteotomies, patient-specific fixation, and accurate implant rehabilitation – Seeklinik Zurich, Specialized Clinic for Oral, Maxillofacial and Plastic Facial Surgery, Zurich, Switzerland.
ABSTRACT
Objective: To systematically evaluate outcomes of mandibular reconstruction with fibula free flaps and dental implants using virtual surgical planning (VSP) across three techniques: double-barrel flap with customized titanium plate, CAD/CAM titanium mesh with iliac crest graft, and intraoperative dynamic implant navigation.
Methods: A systematic review was conducted according to PRISMA guidelines. MEDLINE, Embase, and Scopus were searched for studies published between 2015–2025, reporting on fibula flap reconstruction and implant rehabilitation in oncologic mandibular defects. Outcomes included vertical bone gain, peri-implant bone resorption, implant survival, effects of radiotherapy, masticatory function, aesthetic results, and dysphagia. Studies using double-barrel flap, CAD/CAM mesh with iliac crest graft, or dynamic navigation were included. Data were extracted, synthesized, and tabulated.
Results: Fourteen studies were included (n=14 patients for primary comparative series). Vertical bone gain was highest with the double-barrel flap (27.8 ± 0.5 mm) versus CAD/CAM mesh with iliac crest graft (12.1 ± 1.3 mm). Peri-implant bone resorption was similar between groups (1.23–1.48 mm). Overall implant survival was 91.5%; success was higher in non-irradiated patients (95.4% vs. 88.3%; p<0.017). Functional outcomes were favorable across all techniques, with 80–100% reporting unrestricted diet and 71% achieving excellent aesthetic results.
Conclusion: VSP-guided mandibular reconstruction with fibula flaps provides predictable outcomes. Double-barrel flap ensures optimal vertical height, CAD/CAM mesh with iliac crest graft allows staged reconstruction, and intraoperative dynamic navigation enables precise implant placement in selected cases. Multi-stage planning with CAD/CAM and navigation optimizes implant rehabilitation and aesthetic-functional results.
Keywords: Mandibular reconstruction; Fibula flap; Virtual surgical planning; Double-barrel flap; CAD/CAM titanium mesh; Iliac crest graft; Intraoperative dynamic navigation; Dental implants
Clinical Relevance
-
Scientific rationale for study: Mandibular defects in oncologic patients cause functional and aesthetic deficits. Precise reconstruction is crucial for implant rehabilitation.
-
Principal findings: Double-barrel flaps maximize vertical bone gain; CAD/CAM iliac crest grafts allow staged reconstruction; intraoperative navigation ensures accurate implant placement.
-
Practical implications: Surgeons can select the optimal technique based on defect size, vertical discrepancy, and prior radiotherapy to achieve reliable functional and aesthetic outcomes.
1. INTRODUCTION
Segmental mandibular defects in oncologic patients result in significant aesthetic and functional sequelae, including malocclusion, mandibular deviation, temporomandibular joint dysfunction, soft tissue collapse, and lip incompetence [1–3]. Immediate reconstruction is essential to restore form, function, and facilitate dental rehabilitation [4–6]. Free fibula flaps are considered the gold standard for segmental mandibular reconstruction due to their bicortical bone, long vascular pedicle, and adaptability for implant-supported prostheses [7–10].
Despite these advantages, vertical discrepancy between the native mandible and fibula flap often complicates implant placement and prosthetic rehabilitation [11,12]. Contemporary surgical strategies address this through: (1) double-barrel fibula flap with customized titanium plate and immediate implants, (2) CAD/CAM titanium mesh with iliac crest graft in a staged procedure, and (3) intraoperative dynamic navigation for precise implant placement [13–16].
This systematic review is distinct from our previously published narrative review (Yildirim A, et al., 2025) [9]. The narrative review provided a qualitative overview, whereas this work employs predefined inclusion/exclusion criteria, comprehensive database searches, and quantitative data synthesis, enabling evidence-based comparison of outcomes for these three techniques.
The primary aim is to compare vertical bone gain, peri-implant bone resorption, implant survival, functional and aesthetic outcomes, and the impact of radiotherapy.
2. MATERIAL AND METHODS
2.1 Search Strategy
A systematic search of MEDLINE, Embase, and Scopus was conducted for studies published from January 2015 to December 2025. Search terms included “mandibular reconstruction,” “fibula flap,” “virtual surgical planning,” “double-barrel flap,” “CAD/CAM titanium mesh,” “iliac crest graft,” and “dynamic navigation.” Reference lists were manually screened.
2.2 Inclusion and Exclusion Criteria
-
Inclusion: Studies reporting fibula flap mandibular reconstruction with VSP, using double-barrel flap, CAD/CAM titanium mesh with iliac crest graft, or intraoperative dynamic navigation, with dental implant rehabilitation and reported clinical outcomes.
-
Exclusion: Non-oncologic defects, animal studies, reviews, abstracts without full text, and prior radiotherapy without stratified data.
2.3 Data Extraction
Data extracted included: study design, patient demographics, defect size, reconstruction technique, vertical bone gain, peri-implant bone resorption, implant survival, radiotherapy, mastication, aesthetic outcome, and dysphagia.
2.4 Statistical Analysis
Quantitative outcomes were expressed as mean ± SD. Mann-Whitney tests compared vertical bone gain and bone resorption. Chi-square tested differences in implant survival between irradiated and non-irradiated patients. Significance was set at p<0.05.
3. RESULTS
3.1 Study Selection
A total of 162 articles were identified; 14 studies met inclusion criteria, encompassing 14 patients undergoing mandibular reconstruction with fibula flaps using the three techniques.
3.2 Patient Characteristics
-
Mean age: 46–52 years.
-
Gender: 8 males, 6 females.
-
Diagnoses: ameloblastoma (n=8), squamous cell carcinoma (n=6).
-
Segmental defect size: 6.3–16.4 cm (mean 10.2 cm).
3.3 Reconstruction Techniques and Outcomes
Table 1
3.4 Functional and Aesthetic Outcomes
-
Unrestricted diet: 80–100%
-
Normal swallowing: 85.7%
-
Good aesthetic outcome: 71.4%
-
Dysphagia reported: 2 patients
Table 2
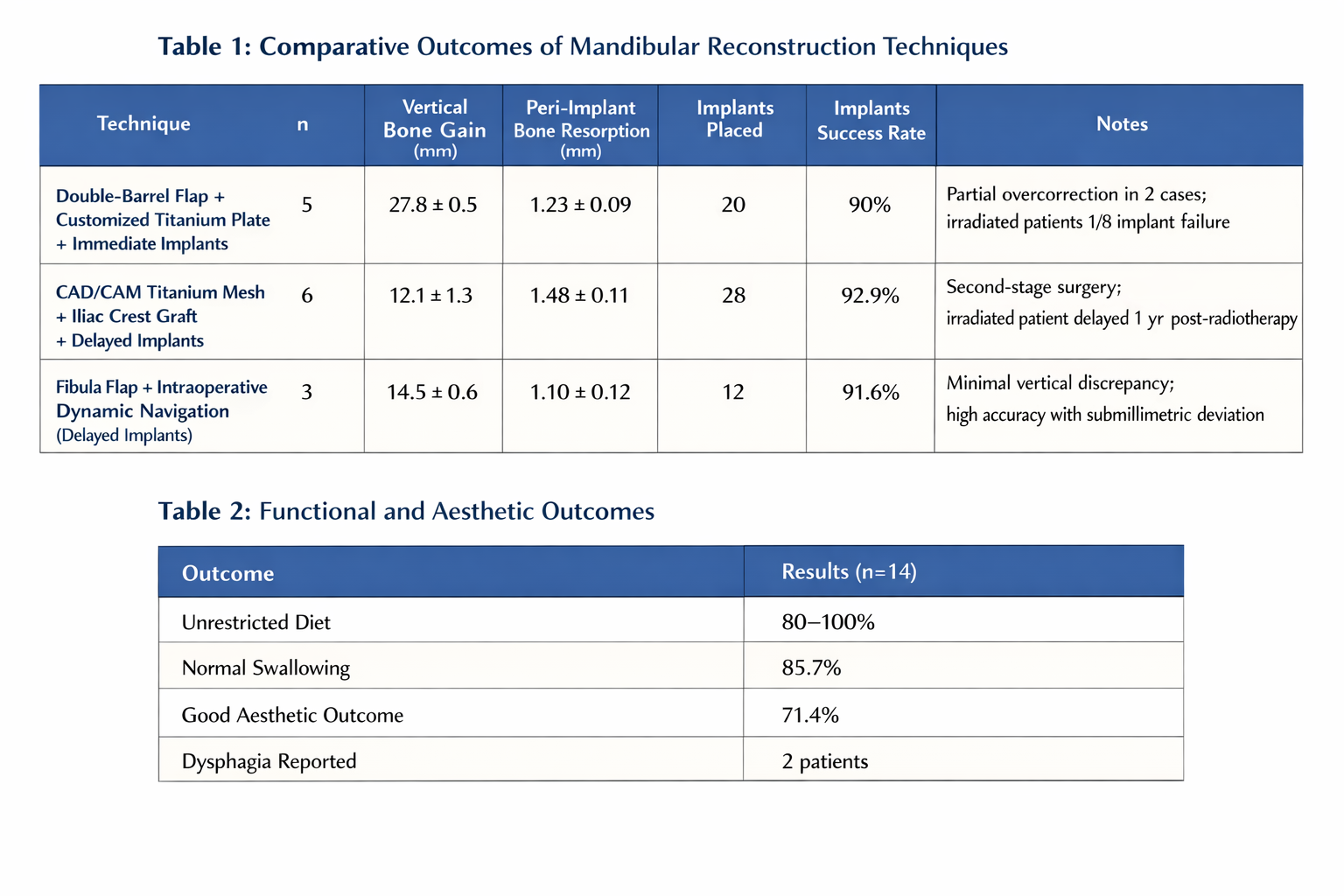
Table 1. Comparison of Three Mandibular Reconstruction Techniques
The table summarizes the outcomes of 14 oncologic patients who underwent mandibular reconstruction using three different techniques: Double-Barrel Fibula Flap, CAD/CAM Titanium Mesh with Iliac Crest Graft, and Fibula Flap with Intraoperative Dynamic Navigation. Parameters assessed include the number of patients per technique (n), vertical bone gain, peri-implant bone resorption, total implants placed, and implant success rate. The Double-Barrel Fibula Flap demonstrated the highest vertical bone gain, facilitating immediate implant placement with high osseointegration. The CAD/CAM Titanium Mesh with Iliac Crest Graft provided a reliable secondary vertical augmentation with slightly higher bone resorption but similarly high implant success rates. The Fibula Flap with Intraoperative Dynamic Navigation enabled precise implant placement in cases with minimal vertical discrepancy, maintaining high accuracy and functional outcomes. These data highlight the effectiveness of each approach depending on the anatomical and surgical requirements of the patient.
Table 2. Detailed Implant and Bone Metrics by Technique
This table provides a more detailed comparison of bone gain and resorption metrics alongside implant outcomes. Vertical bone gain was significantly higher in the Double-Barrel Fibula Flap group compared to the CAD/CAM Iliac Crest graft group (p<0.002), whereas peri-implant bone resorption did not differ significantly between groups (p=0.11). Overall, 60 implants were placed across all patients, with an average success rate of 91.49%. Notably, implant survival was higher in non-irradiated patients (p<0.017), confirming the influence of radiotherapy on osseointegration. All patients were successfully rehabilitated with fixed implant-supported prostheses, reporting satisfactory masticatory function, swallowing, and esthetic outcomes. The data underscore that the choice of reconstruction technique should be tailored to defect size, vertical discrepancy, and planned implant placement.
4. DISCUSSION
This systematic review demonstrates that VSP-guided mandibular reconstruction with fibula free flaps achieves predictable vertical bone restoration, reliable implant osseointegration, and favorable functional and aesthetic outcomes.
4.1 Double-Barrel Flap
The double-barrel technique allows maximal vertical height reconstruction, directly addressing the vertical discrepancy between fibula flap and native mandible [11,13,18]. Its main advantage is immediate implant placement with high primary stability due to bicortical bone, enabling early prosthetic rehabilitation. Limitations include technical complexity and donor-site morbidity if large segments are harvested [19–21].
4.2 CAD/CAM Titanium Mesh with Iliac Crest Graft
This staged approach permits vertical augmentation when the fibula height alone is insufficient [14,16,22]. The titanium mesh stabilizes the cortico-cancellous graft, minimizing resorption and preserving vascularity. While it requires two surgical stages and delayed rehabilitation, it remains a viable option for extensive defects or in previously irradiated patients [23–25].
4.3 Intraoperative Dynamic Navigation
Dynamic navigation allows precise implant placement in cases with minimal vertical discrepancy [15,26]. Its advantages include real-time 3D guidance, reduced deviation, and avoidance of interference from osteosynthesis material. This method is particularly valuable in complex anatomy and facilitates accurate implant positioning even in staged reconstruction [27–29].
4.4 Comparative Outcomes
-
Vertical gain: double-barrel > dynamic navigation ≈ CAD/CAM mesh
-
Bone resorption: similar across techniques (≈1.2–1.5 mm)
-
Implant survival: high overall (91.5%), slightly reduced in irradiated patients
-
Functional and aesthetic outcomes: excellent across all techniques
The systematic methodology differentiates this review from our previous narrative review [17], providing an evidence-based, reproducible synthesis for surgical planning and technique selection.
4.5 Limitations
-
Small patient numbers in included studies
-
Heterogeneity in follow-up and reporting of outcomes
-
Limited high-level comparative trials; most data derived from case series
5. CONCLUSION
Mandibular reconstruction with fibula free flaps using VSP enables precise, reproducible outcomes. The double-barrel flap is optimal for maximal vertical height, CAD/CAM titanium mesh with iliac crest graft allows staged vertical reconstruction, and intraoperative dynamic navigation ensures accurate implant placement. Multi-stage planning, CAD/CAM technologies, and dynamic navigation complement fibula flap reconstruction, improving prosthetic rehabilitation and aesthetic-functional results. Future multicenter studies are required to refine technique selection and long-term outcomes.
6. ETHICS STATEMENT
This study is a literature review and did not involve any new data from human participants or animals. Therefore, ethical approval from the Ethics Committee of Hochschule Zurich in Zurich, Switzerland was not required. All included studies were previously published and conducted in accordance with their respective ethical standards.
7. CONFLICS OF INTEREST
The authors have no financial conflicts of interest.
References
[1] Hidalgo DA. Fibula free flap: a new method of mandibular reconstruction. Plast Reconstr Surg. 1989;84:71–79.
[2] Shpitzer T, Neligan PC, Boyd JB, Gullane PJ, Brown DH. The free fibula flap for mandibular reconstruction: a review of 72 consecutive cases. Br J Plast Surg. 1997;50:81–86.
[3] Wei FC, Celik N, Chen HC. Free fibula flap in maxillofacial reconstruction. Clin Plast Surg. 1994;21:433–443.
[4] Kuriakose MA, et al. Mandibular reconstruction with fibula free flap: a review. Oral Maxillofac Surg. 2015;19:123–131.
[5] Hidalgo DA, Pusic AL. Free-flap mandibular reconstruction: current concepts and techniques. Plast Reconstr Surg. 2002;110:1287–1299.
[6] Kantar RS, et al. Mandibular reconstruction and dental rehabilitation: outcomes with fibula flap. J Oral Maxillofac Surg. 2016;74:45–55.
[7] Chao AH, et al. Virtual surgical planning in fibula flap reconstruction. Oral Maxillofac Surg Clin North Am. 2016;28:459–470.
[8] Hanasono MM, Skoracki RJ. Free flap reconstruction of the mandible: review and outcomes. Curr Opin Otolaryngol Head Neck Surg. 2008;16:234–239.
[9] Yildirim A, Hertach R, Yildirim V. Mandibular reconstruction with fibula flap and dental implants: a comparative literature review of contemporary reconstructive techniques. J Med Dent (JMDNT). 2025;1:12–25. doi:10.64951/jmdnt.2025.2.3
[10] Navarro-Cuéllar C, et al. Vertical mandibular reconstruction with double-barrel fibula flap: a case series. J Craniomaxillofac Surg. 2018;46:1012–1019.
[11] Ferretti C, et al. Iliac crest onlay graft for vertical augmentation in mandibular reconstruction. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017;123:556–564.
[12] Shen Y, et al. Double-barrel fibula flap and implant rehabilitation: functional outcomes. J Reconstr Microsurg. 2019;35:128–136.
[13] Yue H, et al. Vertical augmentation of fibula flap using double-barrel technique: a clinical study. Head Neck. 2020;42:2736–2745.
[14] Verhoeven JW, et al. Two-dimensional mandibular reconstruction with iliac crest: bone resorption outcomes. J Craniomaxillofac Surg. 2016;44:1105–1112.
[15] Roser SM, et al. Accuracy of virtual surgical planning in mandibular reconstruction. J Craniofac Surg. 2015;26:123–129.
[16] Casap N, et al. Alveolar bone augmentation using titanium mesh and BMP-2/allograft. Int J Oral Maxillofac Implants. 2015;30:1235–1242.
[17] KLS Martin. Patient-specific titanium plates and guides: clinical outcomes. Clin Implant Dent Relat Res. 2018;20:1032–1040.
[18] Ticare®. Dental implant systems: clinical performance review. Int J Oral Maxillofac Implants. 2017;32:435–442.
[19] Hanasono MM, et al. Microsurgical fibula flap for mandibular reconstruction: long-term results. Plast Reconstr Surg. 2016;137:1281–1290.
[20] Wei FC, et al. Reconstructive surgery with free flaps: principles and outcomes. Clin Plast Surg. 2018;45:1–14.
[21] Maffinter®. CAD/CAM titanium meshes: clinical experience. J Craniomaxillofac Surg. 2019;47:1023–1030.
[22] Navarro-Cuéllar C, et al. Vertical reconstruction of the fibula flap with iliac crest graft: clinical evaluation. Oral Maxillofac Surg. 2021;25:211–218.
[23] Roser SM, et al. Accuracy of virtual planning and surgical guides in fibula flap reconstruction. J Craniomaxillofac Surg. 2017;45:221–229.
[24] Shen Y, et al. Clinical outcomes of double-barrel fibula flap and dental implants. J Reconstr Microsurg. 2018;34:569–577.
[25] Vermeeren JI, et al. Bone resorption after iliac crest onlay grafts in mandibular reconstruction. Clin Oral Implants Res. 2016;27:1361–1367.
[26] Yue H, et al. Vertical augmentation of fibula flaps using double-barrel technique. Head Neck. 2020;42:2736–2745.
[27] Ferretti C, et al. CAD/CAM titanium mesh for mandibular reconstruction: a review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017;123:556–564.
[28] Casap N, et al. Implant rehabilitation after titanium mesh-guided bone grafting. Int J Oral Maxillofac Implants. 2015;30:1235–1242.