Volume 1, Issue 1, Case Report – May 12, 2025, Pages 12-15,
DOI: 10.64951/jmdnt.2025.1.2
Modified micro-marsupialization as an alternative treatment for ranulas
Ayhan Yildirim¹, René Hertach², Vedat Yildirim¹
¹ Hochschule Zurich, Department of Medicine, Albisstrasse 80, 8038 Zurich, Switzerland
² Hochschule Zurich, Department of Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland
Received 13 November 2024, Revised 14 March 2025, Accepted 25 April 2025, Available online 12 May 2025, Version of Record 12 May 2025.
© 2025 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
ABSTRACT
The anatomical location of ranulas poses an enormous treatment challenge for the dentist. Due to a number of elementary structures, the regional complexity of the area requires a very high level of expertise on the part of the practitioner. The correction of surgical interventions in this area requires great effort. Although complete excision with removal of the sublingual gland remains the gold standard of treatment, recent literature highlights successful results through simple modification of the conventional technique of granular marsupialization. This micromarsupialization option is minimally invasive and beneficial due to the shorter procedure time, minimal discomfort, and lack of postoperative complications. The following case report highlights the successful management of a case using a modified micro-marsupialization technique in an adult.
1. INTRODUCTION
Ranulas are rare mucoceles found on the floor of the mouth. The treatment of ranulas is a challenging and divisive issue. There are still conflicting statements about which treatment method is best. The standard procedure used today is complete excision of the lesion together with excision of the sublingual gland. This intervention ensures a high level of protection against recurrence, as advocated by Pandit and Park [1]. Epidemiologically, these lesions are most common in the first two decades of life; therefore, the treatment approach is generally conservative. In this regard, there have been developments over the last three decades regarding modification of the marsupialization technique that have drastically reduced the likelihood of recurrence [2].
2. CLINICAL CASE REPORT
A 43-year-old man presented to the Seeklinik Zürich, a specialist clinic for oral and maxillofacial surgery and facial plastic surgery, with a feeling of pressure due to swelling on the floor of the left side of the mouth for two weeks.
Two weeks ago, the man noticed a small swelling on the floor of the mouth on the left, which expanded to the size of a cherry in circumference.
The swelling was painless, with no associated dysphagia, paraesthesia or anaesthesia. The man noticed a slight change in the size of the existing swelling, especially during and after meals. Intraoral examination revealed a prominent swelling on the left side of the floor of the mouth, measuring approximately 2 cm × 2 cm × 1.5 cm in length, width and depth. Its anteroposterior margin extended from the mesial surface of the mandibular first molar to the distal aspect of the mandibular lateral incisor. The swelling appeared translucent, reddish and dome-shaped, with some fluid retention therein. No secondary changes, such as ulceration, fistula formation, infection or discharge, were observed [Figure 1].
No similar swelling had been noted in the past, and the medical history was unremarkable. There was no associated head and neck swelling.

Figure 1: Preoperative view
3. CONSENT AND CLINICAL TECHNIQUE
The patient was informed about the various treatment options in such a case, and he decided on the least invasive treatment method. The patient gave written informed consent.
The area was disinfected with a 0.1% povidone iodine solution. The affected area was anesthetized with an inferior alveolar nerve block. Four interrupted sutures of 1-0 silk were passed superficially through the lesion and secured with loose knots [Figure 2]. The patient was instructed to maintain good oral hygiene and to rinse with chlorhexidine mouth rinses twice daily. Follow-up was performed weekly to determine if the sutures were still in place and if the patient was maintaining satisfactory oral hygiene. On the second day, 1 stitch had already been lost. The remaining three sutures were removed after 30 days as described by Matondkar et al. [3]. It was observed that the lesion had already subsided without complications in the first week and did not reappear thereafter. Currently, over nine months have passed since the procedure, with no evidence of recurrence of the lesion [Figure 3].

Figure 2: Post suture placement
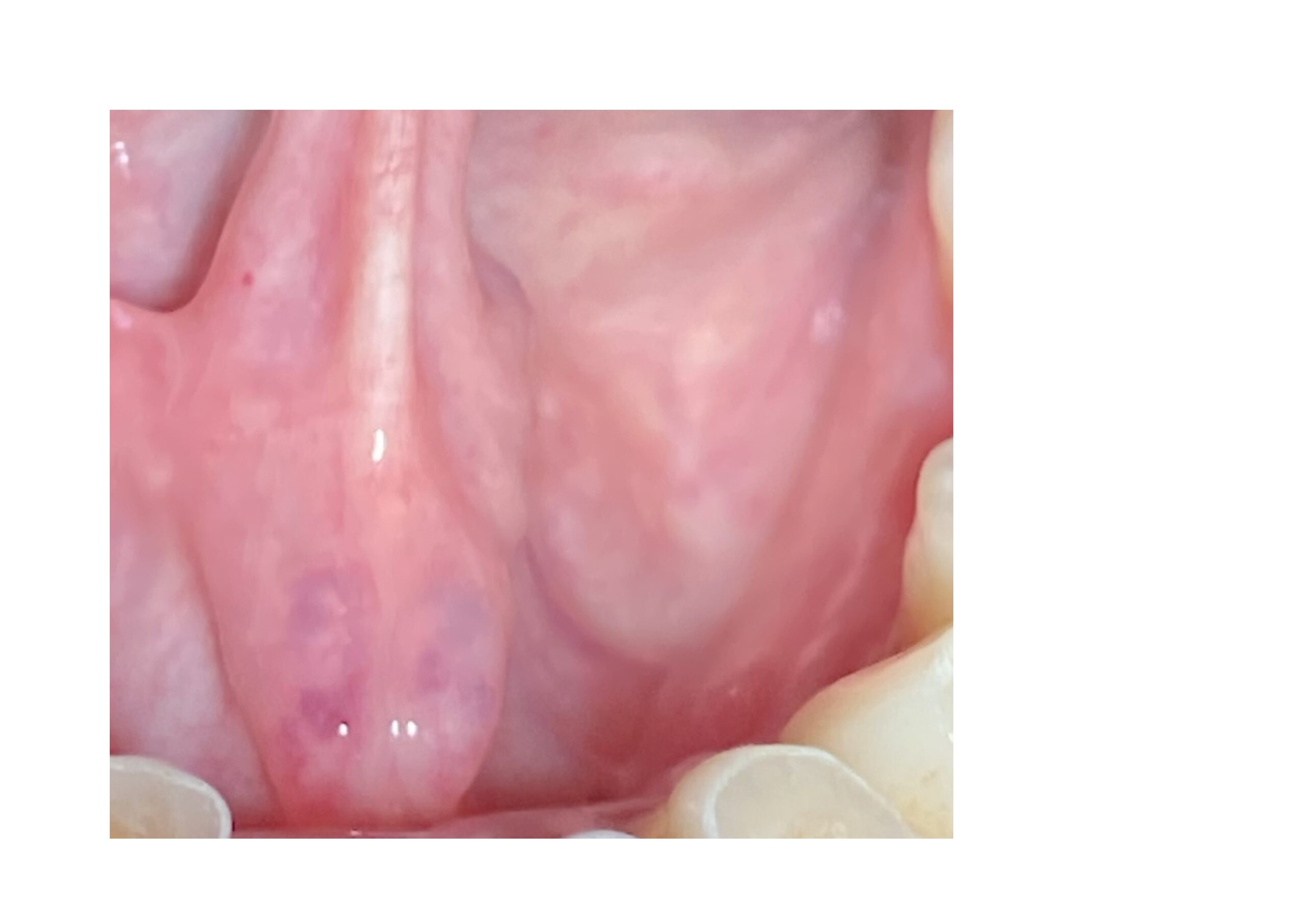
Figure 3: Nine months postoperative
4. DISCUSSION
Ranulas are a rare disease that occurs mainly in the first two decades of life and is a going concern for every dentist. Ranulas typically have a high risk of recurrence. Currently, the only widespread form of therapy is complete excision with removal of the sublingual gland [4]. It should be mentioned that this therapy option is associated with numerous complications and risks. The difficulties mentioned in every surgical explanation are bleeding/hematoma (1%), neuropathic pain due to damage to the lingual nerve and damage to the Wharton duct (2%). In addition, there is a risk of dehiscence in the mylohyoid muscle, which generally leads to recurrence. There is also a risk of restricted mobility of the tongue due to scarring in the surgical site [5]. The surgical field requires careful hygiene postoperatively to prevent secondary infection.
In 1995, Morton and Bartley began to modify the conventional marsupialization approach, placing a single suture of silk on the dome of the ranula.
In 2000, Delbem et al. reported the successful use of a micro-marsupialization technique in the successful treatment of 38 cases of mucus retention phenomena at different sites. The procedure involved the use of a single 4-0 silk suture across the inner portion of the lesion to its widest diameter. This suture was maintained for a week [6].
However, reports of recurrences within 30 days of surgery have appeared in the literature [3]; therefore, this micro-marsupialization technique has undergone further modifications.
In 2007, Sandrini et al. made additional modifications by increasing the number of sutures and reducing the distance between the entry and exit of the needle. The residence time of the sutures in the mucosa was increased to 30 days. Care was taken in tightening the knots to avoid tissue necrosis due to stagnation of blood flow. The mechanism of action in the placement of the large silk suture over a 30-day period is the formation of new, durably epithelialized pathways that serve as additional outlets for the release of the retained mucus [7].
Patient selection plays an important role in the success of therapy. It should not be used in large ranulas that completely fill the floor of the mouth or where the site of origin is difficult to locate [8]. However, it appears to be an ideal approach in cases involving primary lesions up to 4–5 mL in volume. The number of sutures depends on the size of the ranula. The seams should be about 1cm apart. Very thick silk sutures should be made with 1-0 silk so that the epithelization of the replacement duct should be as wide as possible.
5. CONCLUSION
The discussion of the aforementioned procedure underscores the fact that a modified micro-marsupialization technique is a viable alternative to other, more invasive, techniques. The benefits of the procedure are that it is a quick, easy, chairside procedure with minimal postoperative discomfort and complications. As such, it should be explored further as an alternative treatment. The technique definitely deserves wider application.
References
[1] Pandit, R.T. and A.H. Park, Management of pediatric ranula. Otolaryngol Head Neck Surg, 2002. 127(1): p. 115-8.
[2] Baurmash, H.D., Treating oral ranula: another case against blanket removal of the sublingual gland. Br J Oral Maxillofac Surg, 2001. 39(3): p. 217-20.
[3] Matondkar, S.P., C. Yavagal, and P.S. Mandroli, Modified micro-marsupialization as an alternative treatment for the management of ranulas in children. Natl J Maxillofac Surg, 2019. 10(1): p. 95-97.
[4] Crysdale, W.S., J.D. Mendelsohn, and S. Conley, Ranulas–mucoceles of the oral cavity: experience in 26 children. Laryngoscope, 1988. 98(3): p. 296-8.
[5] . Zhao, Y.F., J. Jia, and Y. Jia, Complications associated with surgical management of ranulas. J Oral Maxillofac Surg, 2005. 63(1): p. 51-4.
[6] Delbem, A.C., et al., Treatment of mucus retention phenomena in children by the micro-marsupialization technique: case reports. Pediatr Dent, 2000. 22(2): p. 155-8.
[7] Sandrini, F.A., M. Sant’ana-Filho, and P.V. Rados, Ranula management: suggested modifications in the micro-marsupialization technique. J Oral Maxillofac Surg, 2007. 65(7): p. 1436-8.
[8] Goodson, A.M., et al., Minimally invasive treatment of oral ranulae: adaption to an old technique. Br J Oral Maxillofac Surg, 2015. 53(4): p. 332-5.