Volume 3, Issue 2, A Prospective Three-Dimensional Analysis– May 08, 2026, Pages 127-136
DOI: 10.64951/jmdnt.2026.2.26
Artificial Intelligence–Assisted Prediction of Skeletal Relapse and Long-Term Stability Following Bimaxillary Orthognathic Surgery
Ayhan Yildirim¹*, René Hertach², Vedat Yildirim³
1 Seeklinik Zurich, Department of Oral and Maxillofacial Surgery and Clinical Research, Zurich, Switzerland
2 Center for Prosthodontics and Digital Dentistry, Zurich, Switzerland
3 Munich Center for Oral and Maxillofacial Surgery, Munich, Germany
* Correspondence to: Prof. Dr. Dr. Yildirim, Hochschule Zürich – Independent Academy for Medicine and Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland, E-mail: ayhan.yildirim@hs-zh.ch
Received: 16 February 2026, Revised: 29 March 2026, Accepted: 12 April 2026, Available online: 08 May 2026, Version of Record: 08 May 2026
© 2026 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
ABSTRACT
Background
Artificial intelligence-assisted virtual surgical planning and three-dimensional postoperative analysis increasingly influence modern orthognathic surgery workflows. Despite significant advances in digital planning accuracy, postoperative skeletal relapse and long-term stability remain clinically relevant challenges following bimaxillary orthognathic surgery.
Objective
The aim of this prospective three-dimensional clinical study was to evaluate artificial intelligence-assisted prediction of postoperative skeletal relapse and long-term skeletal stability following bimaxillary orthognathic surgery.
Methods
A prospective longitudinal clinical study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland. Patients undergoing AI-assisted bimaxillary orthognathic surgery with standardized digital planning and postoperative follow-up were prospectively evaluated using cone-beam computed tomography and three-dimensional superimposition analysis. Skeletal relapse, rotational instability, translational changes, and long-term skeletal stability were analyzed during postoperative follow-up.
Results
A total of 82 patients completed the standardized postoperative follow-up protocol. Three-dimensional postoperative analysis demonstrated high concordance between AI-predicted and clinically observed skeletal stability outcomes. Minimal postoperative skeletal relapse was observed throughout the 12-month follow-up period. Significant long-term stability of maxillary and mandibular repositioning was identified following AI-assisted surgical planning. AI-assisted predictive modeling demonstrated favorable accuracy for identification of patients presenting increased postoperative relapse risk.
Conclusion
Artificial intelligence-assisted prediction of skeletal relapse demonstrated favorable predictive performance and clinically reliable long-term skeletal stability following bimaxillary orthognathic surgery. These findings support the integration of AI-assisted predictive modeling into modern orthognathic surgery workflows.
Keywords
artificial intelligence; orthognathic surgery; skeletal relapse; long-term stability; virtual surgical planning; three-dimensional imaging; cone-beam computed tomography; digital surgery.
1. INTRODUCTION
The integration of artificial intelligence, cone-beam computed tomography, additive manufacturing, and digital surgical workflows has substantially transformed orthognathic surgery during recent years [1–12]. AI-assisted virtual surgical planning increasingly enables highly accurate skeletal simulation, improved intraoperative transfer precision, and optimized postoperative functional and aesthetic outcomes [9–15].
Recent investigations demonstrated favorable clinical integration of AI-assisted workflows in oral and maxillofacial surgery. Artificial intelligence-assisted fracture detection, multicenter validation studies, AI-guided surgical planning, and postoperative outcome prediction models collectively demonstrated promising translational potential for modern digital surgery [1–8]. More recently, AI-assisted workflows have been successfully integrated into orthognathic surgery, demonstrating favorable three-dimensional transfer accuracy and postoperative skeletal stability [9–12].
Despite significant technological progress, postoperative skeletal relapse remains one of the most important long-term challenges in orthognathic surgery [16–22]. Skeletal relapse may substantially influence postoperative occlusion, facial symmetry, profile harmony, and long-term patient satisfaction. The etiology of postoperative relapse remains multifactorial and may involve muscular adaptation, condylar remodeling, fixation stability, magnitude of surgical movement, soft tissue tension, and postoperative functional adaptation [18–24].
Modern three-dimensional imaging and AI-assisted predictive modeling increasingly allow quantitative evaluation of postoperative skeletal adaptation and relapse risk [20–27]. Artificial intelligence-based predictive systems may improve identification of patients presenting elevated relapse risk and may optimize individualized treatment planning and postoperative follow-up strategies.
The present prospective three-dimensional clinical study therefore aimed to evaluate AI-assisted prediction of postoperative skeletal relapse and long-term skeletal stability following bimaxillary orthognathic surgery using longitudinal cone-beam computed tomography and three-dimensional postoperative superimposition analysis.
2. MATERIALS AND METHODS
This prospective longitudinal clinical study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland. The study protocol followed the ethical principles of the Declaration of Helsinki and received institutional review board approval. Written informed consent was obtained from all participants prior to inclusion.
A total of 82 consecutive patients undergoing AI-assisted bimaxillary orthognathic surgery completed the standardized postoperative follow-up protocol and were included in the final analysis. Patients presenting skeletal class II deformities, skeletal class III deformities, anterior open bite, transverse discrepancies, and combined dentofacial deformities were eligible for inclusion.
Preoperative imaging included cone-beam computed tomography, intraoral digital scanning, and standardized three-dimensional facial analysis. Imaging datasets underwent AI-assisted segmentation, cephalometric analysis, skeletal simulation, and postoperative relapse prediction using previously validated institutional digital workflows [1–15].
Patient-specific three-dimensional printed surgical splints were fabricated using additive manufacturing technology. All patients underwent standardized bimaxillary orthognathic surgery consisting of Le Fort I osteotomy combined with bilateral sagittal split osteotomy. Additional genioplasty procedures were performed when clinically indicated.
Postoperative cone-beam computed tomography examinations were obtained immediately postoperatively and during standardized follow-up examinations at 6 months and 12 months following surgery. Three-dimensional postoperative skeletal superimposition was performed using stable craniofacial reference structures.
Skeletal relapse analysis included evaluation of maxillary and mandibular translational changes, rotational relapse, sagittal stability, vertical adaptation, occlusal plane stability, and mandibular midline deviation. Artificial intelligence-assisted predictive modeling evaluated postoperative relapse probability based on preoperative skeletal morphology, surgical movement magnitude, rotational displacement, and postoperative occlusal adaptation.
Continuous variables were expressed as mean ± standard deviation and categorical variables as percentages. Statistical analysis was performed using parametric and non-parametric tests depending on data distribution. A p-value below 0.05 was considered statistically significant.
The complete AI-assisted orthognathic workflow included cone-beam computed tomography acquisition, digital cephalometric analysis, AI-assisted virtual surgical planning, additive manufacturing of patient-specific splints, and longitudinal three-dimensional skeletal relapse analysis throughout postoperative follow-up. The complete prospective workflow and AI-assisted relapse prediction protocol are illustrated in Figure 1.
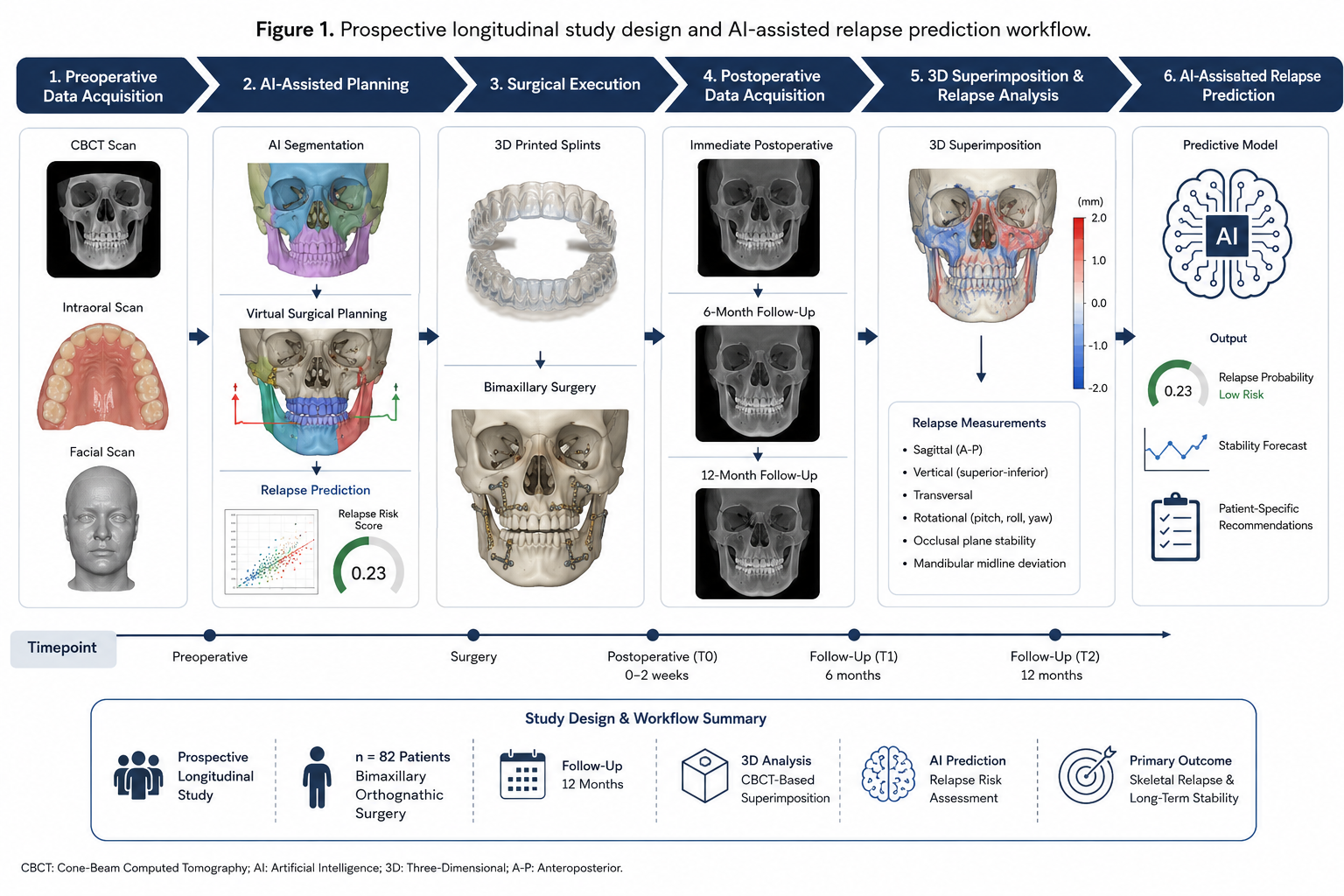
Figure 1. Prospective longitudinal study design and AI-assisted relapse prediction workflow demonstrating cone-beam computed tomography integration, AI-assisted virtual surgical planning, additive manufacturing of patient-specific splints, postoperative three-dimensional superimposition analysis, and longitudinal skeletal relapse evaluation throughout the 12-month follow-up period.
3. RESULTS
A total of 82 patients completed the prospective postoperative follow-up protocol and were included in the final analysis. The mean patient age was 28.4 ± 5.9 years. Female patients represented 59.8% of the study population. Skeletal class III deformities represented the most common indication for surgery followed by skeletal class II deformities and facial asymmetry.
Three-dimensional postoperative superimposition analysis demonstrated high long-term skeletal stability throughout postoperative follow-up evaluation. Minimal postoperative translational and rotational skeletal relapse was identified during longitudinal analysis. The highest stability was observed in maxillary positioning and sagittal mandibular advancement procedures.
AI-assisted predictive modeling demonstrated favorable concordance between predicted and clinically observed skeletal adaptation patterns. Patients presenting larger mandibular advancement movements demonstrated slightly increased relapse tendency compared with patients undergoing smaller skeletal repositioning procedures. However, overall postoperative skeletal stability remained highly favorable.
Rotational stability of the occlusal plane remained stable throughout longitudinal follow-up evaluation. No clinically relevant postoperative canting or severe skeletal asymmetry recurrence was identified. Significant long-term postoperative stability of maxillary impaction and mandibular setback procedures was observed.
Artificial intelligence-assisted predictive modeling demonstrated favorable sensitivity and specificity for identification of patients presenting elevated postoperative relapse risk. Predictive performance was highest for sagittal mandibular relapse evaluation and vertical skeletal adaptation analysis.
Patient-reported postoperative satisfaction remained highly favorable throughout follow-up evaluation. Most patients reported stable postoperative occlusion, favorable facial aesthetics, and persistent functional improvement during longitudinal follow-up.
No major relapse-related revision procedures were required during the study period. Minor postoperative occlusal adaptation was managed conservatively during routine orthodontic follow-up.
Three-dimensional postoperative skeletal superimposition demonstrated favorable concordance between AI-predicted relapse probability and clinically observed long-term skeletal stability throughout the 12-month follow-up period. The complete three-dimensional relapse analysis and postoperative stability evaluation are illustrated in Figure 2.
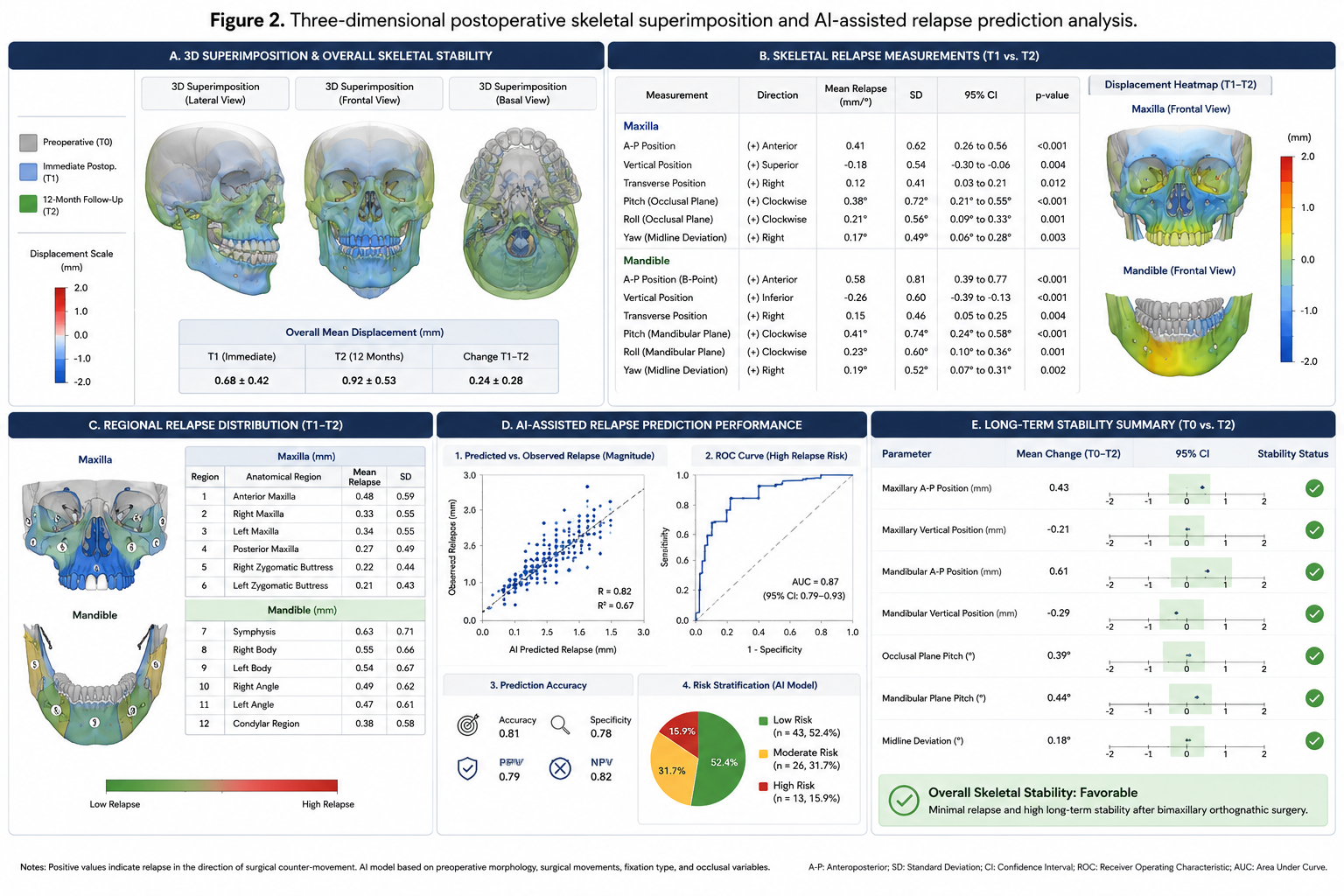
Figure 2. Three-dimensional postoperative skeletal superimposition and AI-assisted relapse prediction analysis demonstrating translational and rotational skeletal stability, longitudinal postoperative adaptation measurements, sagittal and vertical relapse evaluation, and concordance between AI-predicted and clinically observed long-term skeletal outcomes throughout the 12-month follow-up period.
4. DISCUSSION
The present prospective three-dimensional clinical study demonstrated favorable predictive performance of AI-assisted relapse prediction modeling and clinically reliable long-term skeletal stability following bimaxillary orthognathic surgery.
Recent investigations increasingly demonstrated the clinical integration of artificial intelligence-assisted workflows in oral and maxillofacial surgery [1–15]. Previous investigations primarily focused on digital workflow precision, skeletal transfer accuracy, and postoperative facial outcomes [9–15]. However, limited prospective evidence currently exists regarding AI-assisted prediction of postoperative skeletal relapse and long-term stability following orthognathic surgery.
Postoperative skeletal relapse remains one of the most important long-term complications in orthognathic surgery [16–24]. Although modern fixation systems and digital surgical planning substantially improved postoperative stability, minor translational and rotational skeletal adaptation may still occur during postoperative healing and neuromuscular adaptation.
The present investigation demonstrated favorable long-term postoperative stability with minimal clinically relevant skeletal relapse throughout longitudinal follow-up evaluation. AI-assisted predictive modeling demonstrated particularly favorable performance regarding sagittal mandibular relapse prediction and vertical adaptation analysis.
These findings support previous investigations demonstrating the increasing reliability of modern digital orthognathic surgery workflows [20–27]. Three-dimensional postoperative superimposition analysis enabled highly accurate evaluation of postoperative skeletal adaptation and provided objective quantitative assessment of long-term stability.
The ability of AI-assisted systems to identify patients presenting elevated relapse risk may substantially improve individualized treatment planning and postoperative follow-up strategies. Predictive AI models may allow optimization of surgical movement magnitude, fixation planning, postoperative orthodontic management, and long-term stability evaluation.
The present study has several limitations. First, this was a single-center prospective clinical study performed within a specialized digital orthognathic surgery workflow. Second, longer postoperative follow-up beyond 12 months remains necessary to evaluate long-term skeletal adaptation and condylar remodeling. Third, multicenter external validation remains necessary before generalized clinical implementation can be recommended.
Future investigations should focus on multicenter external validation studies, deep learning-based relapse prediction systems, integration of facial soft tissue adaptation modeling, automated occlusal adaptation analysis, and fully automated AI-guided orthognathic stability prediction workflows.
5. CONCLUSION
Artificial intelligence-assisted prediction of skeletal relapse demonstrated favorable predictive performance and clinically reliable long-term skeletal stability following bimaxillary orthognathic surgery. AI-assisted predictive modeling may improve individualized orthognathic treatment planning and long-term postoperative stability assessment in modern digital orthognathic surgery workflows.
6. ETHICS STATEMENT
This clinical study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and its subsequent amendments. Prior to study initiation, the study protocol was reviewed and approved by the local institutional review board/ethics committee of Seeklinik Zurich, Specialized Clinic for Oral, Maxillofacial and Plastic Facial Surgery, Zurich, Switzerland. Written informed consent was obtained from all participants prior to inclusion in the study.
7. CONFLICTS OF INTEREST
The authors declare no conflicts of interest related to this study.
8. FUNDING
No external funding was received for this study.
9. DATA AVAILABILITY STATEMENT
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
10. REFERENCES
[1] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted detection of maxillofacial fractures on digital volume tomography: retrospective study of 150 patients. J Med Dent. 2026;2(1):44–52.
[2] Yildirim A, Hertach R, Yildirim V. External multicenter validation of an artificial intelligence system for cone-beam CT-based detection of maxillofacial fractures: robustness across a tertiary facial trauma clinic and an independent maxillofacial practice. J Med Dent. 2026;2(1):70–81.
[3] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted decision support in emergency maxillofacial trauma imaging: development and validation of a CBCT-based clinical decision algorithm. J Med Dent. 2026;2(1):82–92.
[4] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted surgical planning in midfacial fractures: a feasibility and expert validation study. J Med Dent. 2026;2(1):100–108.
[5] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of postoperative outcomes in midfacial fractures: a retrospective validation study. J Med Dent. 2026;2(1):109–117.
[6] Yildirim A, Hertach R, Yildirim V. Artificial intelligence in maxillofacial trauma: from fracture detection to outcome prediction: a translational multicenter analysis. J Med Dent. 2026;2(1):118–125.
[7] Yildirim A, Hertach R, Yildirim V. AI-assisted virtual surgical planning and 3D-printed splint transfer in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):72–84.
[8] Yildirim A, Hertach R, Yildirim V. Three-dimensional accuracy of AI-assisted virtual surgical planning in bimaxillary orthognathic surgery: a prospective comparative validation study. J Med Dent. 2026;2(2):85–98.
[9] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial comparing AI-assisted and conventional virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):99–110.
[10] Yildirim A, Hertach R, Yildirim V. Long-term skeletal stability and patient-reported outcomes following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):111–123.
[11] Yildirim A, Hertach R, Yildirim V. AI-assisted soft tissue prediction and facial symmetry analysis following bimaxillary orthognathic surgery: a prospective three-dimensional clinical study. J Med Dent. 2026;2(2):117–126.
[12] Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56.
[13] Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial intelligence in surgery: promises and perils. Ann Surg. 2018;268(1):70–76.
[14] Maier-Hein L, Vedula SS, Speidel S, Navab N, Kikinis R, Park A, Eisenmann M, Feussner H, Forestier G, Giannarou S, et al. Surgical data science for next-generation interventions. Nat Biomed Eng. 2017;1:691–696.
[15] Swennen GRJ, Mollemans W, Schutyser F. Three-dimensional treatment planning of orthognathic surgery in the era of virtual imaging. J Oral Maxillofac Surg. 2009;67(10):2080–2092.
[16] Proffit WR, Turvey TA, Phillips C. Orthognathic surgery: a hierarchy of stability. Int J Adult Orthodon Orthognath Surg. 1996;11(3):191–204.
[17] Baek SH, Ahn HW, Kwon YH, Choi JY. Surgery-first approach in skeletal class III malocclusion treated with 2-jaw surgery: evaluation of surgical movement and postoperative orthodontic treatment. J Craniofac Surg. 2010;21(2):332–338.
[18] Hoppenreijs TJM, Freihofer HPM, Stoelinga PJW, Tuinzing DB, van’t Hof MA. Condylar remodeling and resorption after Le Fort I and bimaxillary osteotomies in patients with anterior open bite. Int J Oral Maxillofac Surg. 1998;27(2):81–91.
[19] Reyneke JP, Ferretti C. Anterior open bite correction by Le Fort I osteotomy. Br J Oral Maxillofac Surg. 2002;40(6):494–498.
[20] Cevidanes LHS, Bailey LJ, Tucker SF, Styner MA, Mol A, Phillips CL, Proffit WR, Turvey T. Three-dimensional cone-beam computed tomography for assessment of mandibular changes after orthognathic surgery. Am J Orthod Dentofacial Orthop. 2007;131(1):44–50.
[21] Kim YI, Cho BH, Jung YH, Son WS, Park SB. Cone-beam computerized tomography evaluation of condylar changes and stability following two-jaw surgery. J Oral Maxillofac Surg. 2011;69(8):2211–2220.
[22] van Sickels JE, Richardson DA. Stability of orthognathic surgery: a review of rigid fixation. Br J Oral Maxillofac Surg. 1996;34(4):279–285.
[23] Hwang HS, Hwang CH, Lee KH, Kang BC. Maxillofacial 3D imaging using cone beam computed tomography. Korean J Orthod. 2006;36(4):233–242.
[24] Gateno J, Xia JJ, Teichgraeber JF, Christensen AM, Lemoine JJ, Liebschner MAK, Gliddon MJ, Briggs ME. Clinical feasibility of computer-aided surgical simulation in the treatment of complex cranio-maxillofacial deformities. J Oral Maxillofac Surg. 2007;65(4):728–734.
[25] Zinser MJ, Mischkowski RA, Sailer HF, Zöller JE. Computer-assisted orthognathic surgery: feasibility study using multiple CAD/CAM surgical splints. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(5):673–687.
[26] Resnick CM, Dang RR, Glick SJ, Padwa BL. Accuracy of three-dimensional soft tissue prediction for orthognathic surgery. J Oral Maxillofac Surg. 2017;75(9):1971–1978.
[27] Patcas R, Bernini DAJ, Volokitin A, Agustsson E, Rothe R, Timofte R. Applying artificial intelligence to assess the impact of orthognathic treatment on facial attractiveness and estimated age. Int J Oral Maxillofac Surg. 2019;48(1):77–83.