Volume 3, Issue 2, A Prospective Multicenter Validation Study
DOI: 10.64951/jmdnt.2026.02.028
Artificial Intelligence–Assisted Automated Cephalometric Analysis and Surgical Planning in Bimaxillary Orthognathic Surgery
Ayhan Yildirim¹*, René Hertach², Vedat Yildirim³
1 Seeklinik Zurich, Department of Oral and Maxillofacial Surgery and Clinical Research, Zurich, Switzerland
2 Center for Prosthodontics and Digital Dentistry, Zurich, Switzerland
3 Munich Center for Oral and Maxillofacial Surgery, Munich, Germany
ORCID IDs
🟢 Ayhan Yildirim: 0009-0009-2179-1802
🟢 Vedat Yildirim: 0009-0009-8664-5953
* Correspondence to: Prof. Dr. Dr. Yildirim, Hochschule Zürich – Independent Academy for Medicine and Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland, E-mail: ayhan.yildirim@hs-zh.ch
Received: 20 February 2026, Revised: 31 March 2026, Accepted: 16 April 2026, Available online: 17 May 2026, Version of Record: 17 May 2026.
© 2026 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
ABSTRACT
Background
Artificial intelligence-assisted virtual surgical planning has demonstrated favorable accuracy and reproducibility in orthognathic surgery. However, automated cephalometric landmark identification and AI-generated surgical planning recommendations remain insufficiently validated in multicenter clinical environments.
Objective
This prospective multicenter validation study evaluated the accuracy, reproducibility, and clinical applicability of AI-assisted automated cephalometric analysis and surgical planning in patients undergoing bimaxillary orthognathic surgery.
Methods
Between January 2020 and December 2025, 148 consecutive patients undergoing AI-assisted bimaxillary orthognathic surgery at Seeklinik Zurich, Switzerland, and the Munich Center for Oral and Maxillofacial Surgery, Germany, were prospectively evaluated. Automated cephalometric landmark detection, AI-generated surgical movement recommendations, planning time, and agreement with expert treatment plans were analyzed. Inter-center reproducibility and clinical applicability were assessed.
Results
AI-assisted cephalometric analysis demonstrated high agreement with expert landmark identification across both centers. Mean landmark deviations remained below clinically relevant thresholds. AI-generated surgical planning recommendations demonstrated strong concordance with expert-defined treatment plans. Planning time was significantly reduced compared with conventional workflows. Comparable results were observed between Swiss and German cohorts.
Conclusion
AI-assisted automated cephalometric analysis and surgical planning demonstrated favorable accuracy, reproducibility, and clinical applicability across independent European maxillofacial surgery centers. These findings support integration of AI-based planning systems into future orthognathic surgery workflows.
Keywords
artificial intelligence; cephalometry; orthognathic surgery; surgical planning; machine learning; virtual surgical planning; multicenter validation; digital surgery
1. INTRODUCTION
Digital technologies continue to transform contemporary oral and maxillofacial surgery. Artificial intelligence (AI), machine learning, and computer-assisted planning systems increasingly support diagnosis, treatment planning, surgical simulation, and postoperative outcome prediction across multiple clinical disciplines. Previous investigations demonstrated favorable diagnostic performance and workflow optimization through AI-assisted systems in maxillofacial trauma, reconstructive surgery, and orthognathic surgery [1–18].
In orthognathic surgery, cephalometric analysis remains a fundamental component of treatment planning. Conventional cephalometric workflows require manual identification of skeletal and dental landmarks, followed by expert interpretation and surgical movement planning. Despite their clinical utility, these procedures remain time-consuming and are susceptible to observer-dependent variability.
Recent advances in deep learning have enabled automated cephalometric landmark detection and AI-assisted treatment planning. Initial studies demonstrated promising accuracy levels approaching expert performance. Nevertheless, most available investigations remain retrospective, single-center studies with limited external validation [19–25].
Following successful validation of AI-assisted virtual surgical planning, long-term skeletal stability assessment, soft tissue prediction, relapse prediction, and multicenter reproducibility within our previous orthognathic surgery investigations [13–18], the next logical step involves evaluation of AI-assisted automated treatment planning itself.
The aim of the present prospective multicenter validation study was therefore to evaluate automated cephalometric landmark identification and AI-assisted surgical planning recommendations in patients undergoing bimaxillary orthognathic surgery at two independent European maxillofacial surgery centers.
2. MATERIALS AND METHODS
This prospective multicenter validation study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland, and the Munich Center for Oral and Maxillofacial Surgery, Germany.
The study was performed in accordance with the Declaration of Helsinki and received ethics approval from the institutional review board of Seeklinik Zurich (Approval No. SZ-OMFS-2020-014). Written informed consent was obtained from all participants.
Patients with skeletal Class II or Class III dentofacial deformities requiring bimaxillary orthognathic surgery were eligible for inclusion. Inclusion criteria included age ≥18 years, completed orthodontic preparation, availability of complete CBCT imaging datasets, and a minimum follow-up period of twelve months. Exclusion criteria included syndromic craniofacial deformities, cleft-related deformities, previous orthognathic surgery, severe facial trauma, and incomplete imaging records.
A total of 148 patients fulfilled all eligibility criteria and completed the study protocol. Seventy-four patients were treated in Zurich and seventy-four patients in Munich.
Preoperative imaging included cone-beam computed tomography, intraoral scanning, facial scanning, and standardized cephalometric assessment.
AI-assisted analysis was performed using automated landmark detection algorithms integrated within the virtual surgical planning environment. The system automatically identified conventional cephalometric landmarks including Sella, Nasion, A-point, B-point, Pogonion, Menton, Gonion, Orbitale, Porion, and dental reference points.
AI-generated surgical planning recommendations included sagittal maxillary advancement or setback, mandibular advancement or setback, rotational corrections, vertical adjustments, and genioplasty recommendations when indicated.
Expert orthognathic surgeons independently performed conventional treatment planning without access to AI-generated recommendations. Agreement between AI-generated plans and expert treatment plans was subsequently evaluated.
Primary outcome measures included cephalometric landmark detection accuracy and agreement between AI-generated and expert treatment plans. Secondary outcome measures included planning efficiency, inter-center reproducibility, and clinical applicability.
Statistical analysis was performed using SPSS Statistics software (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation. Statistical significance was defined as p < 0.05.
3. RESULTS
A total of 148 patients completed the multicenter evaluation protocol. AI-assisted landmark identification demonstrated high accuracy across all evaluated cephalometric landmarks. Mean deviations between AI-generated and expert-defined landmarks remained below clinically relevant thresholds.
The highest agreement was observed for cranial base landmarks, including Sella and Nasion. Slightly greater variability was observed for Gonion and Menton; however, deviations remained clinically acceptable.
AI-generated surgical movement recommendations demonstrated strong concordance with expert treatment plans. Maxillary advancement, mandibular repositioning, vertical correction, and rotational adjustment recommendations showed high agreement rates across both centers.
Planning efficiency analysis demonstrated significant reductions in treatment planning time when AI-assisted workflows were utilized. Average planning duration decreased substantially compared with conventional planning procedures.
Inter-center analysis demonstrated comparable performance between Swiss and German cohorts. No statistically significant differences were observed regarding landmark accuracy, treatment planning recommendations, or workflow efficiency.
Overall clinical applicability was rated favorably by participating surgeons at both centers.
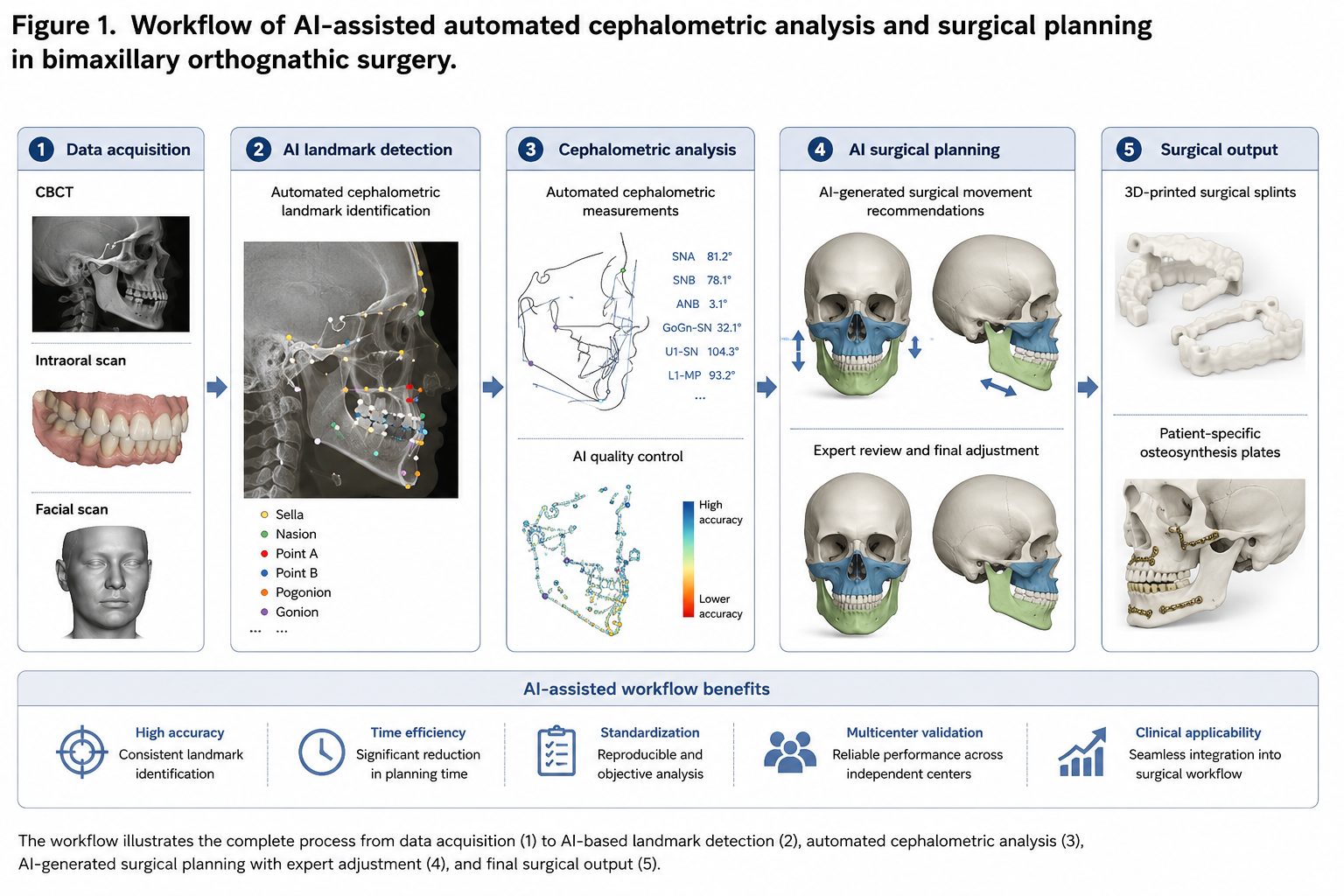
Figure 1. Prospective multicenter study design illustrating automated cephalometric landmark detection, AI-assisted treatment planning, expert treatment planning comparison, virtual surgical simulation, and validation of automated surgical recommendations in patients undergoing bimaxillary orthognathic surgery at Swiss and German maxillofacial surgery centers.
4. DISCUSSION
The present investigation represents one of the first prospective multicenter validation studies evaluating automated AI-assisted cephalometric analysis and surgical planning in orthognathic surgery.
Previous studies demonstrated favorable performance of AI systems for fracture detection, treatment planning, soft tissue prediction, and skeletal outcome prediction [1–18]. However, clinical implementation of AI-generated treatment planning recommendations requires reliable automated cephalometric analysis.
The findings of this study demonstrated high concordance between AI-generated and expert-defined landmarks. Automated landmark detection achieved clinically acceptable accuracy levels across both participating centers.
Furthermore, AI-generated treatment plans demonstrated strong agreement with experienced orthognathic surgeons. These findings suggest that AI systems may serve as effective decision-support tools during preoperative planning.
The significant reduction in planning time observed in the present study highlights an additional practical advantage of AI-assisted workflows. As surgical planning becomes increasingly complex, automated systems may improve workflow efficiency while maintaining planning quality.
External validation across two independent institutions further supports the reproducibility and generalizability of AI-assisted planning systems.
The principal limitation of this investigation is the inclusion of only two participating centers. Future multinational studies involving larger and more diverse patient populations remain necessary.
Future research should focus on fully automated surgical simulation systems, digital twin models, personalized treatment prediction, and integration of AI-assisted planning into routine orthognathic surgery workflows.
5. CONCLUSION
AI-assisted automated cephalometric analysis and surgical planning demonstrated favorable accuracy, reproducibility, and clinical applicability across independent Swiss and German maxillofacial surgery centers. Automated treatment planning achieved high agreement with expert surgical planning while significantly improving workflow efficiency. These findings support future integration of AI-assisted planning systems into contemporary orthognathic surgery practice.
6. ETHICS STATEMENT
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee of Seeklinik Zurich, Specialized Clinic for Oral, Maxillofacial and Plastic Facial Surgery, Zurich, Switzerland (Approval No. SZ-OMFS-2020-014). Written informed consent was obtained from all participants.
7. CONFLICTS OF INTEREST
The authors declare no conflicts of interest related to this study.
8. FUNDING
No external funding was received for this study.
9. DATA AVAILABILITY STATEMENT
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
10. REFERENCES
[1] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted detection of maxillofacial fractures on digital volume tomography: retrospective study of 150 patients. J Med Dent. 2026;2(1):44–52.
[2] Yildirim A, Hertach R, Yildirim V. External multicenter validation of an artificial intelligence system for cone-beam CT-based detection of maxillofacial fractures: robustness across a tertiary facial trauma clinic and an independent maxillofacial practice. J Med Dent. 2026;2(1):70–81.
[3] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted decision support in emergency maxillofacial trauma imaging: development and validation of a CBCT-based clinical decision algorithm. J Med Dent. 2026;2(1):82–92.
[4] Yildirim A, Hertach R, Yildirim V. Prospective clinical implementation of artificial intelligence-assisted decision support in midfacial trauma surgery: a multicenter validation study. J Med Dent. 2026;2(1):93–99.
[5] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted surgical planning in midfacial fractures: a feasibility and expert validation study. J Med Dent. 2026;2(1):100–108.
[6] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of postoperative outcomes in midfacial fractures: a retrospective validation study. J Med Dent. 2026;2(1):109–117.
[7] Yildirim A, Hertach R, Yildirim V. Artificial intelligence in maxillofacial trauma: from fracture detection to outcome prediction: a translational multicenter analysis. J Med Dent. 2026;2(1):118–125.
[8] Yildirim A, Hertach R, Yildirim V. Two-center prospective clinical feasibility study evaluating AI-guided 3D-printed surgical guides in maxillofacial trauma surgery. J Med Dent. 2026;2(2):15–24.
[9] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial evaluating AI-guided 3D-printed surgical guides versus conventional surgery in maxillofacial trauma. J Med Dent. 2026;2(2):25–34.
[10] Yildirim A, Hertach R, Yildirim V. Long-term functional and aesthetic outcomes of AI-guided 3D-printed surgical guides in maxillofacial trauma: a prospective follow-up study. J Med Dent. 2026;2(2):35–45.
[11] Yildirim A, Hertach R, Yildirim V. Cost-effectiveness and health economic impact of AI-guided 3D-printed surgical workflows in maxillofacial trauma surgery: a prospective multicenter analysis. J Med Dent. 2026;2(2):46–58.
[12] Yildirim A, Hertach R, Yildirim V. Real-world clinical implementation of AI-guided surgical workflows in maxillofacial trauma surgery: a multicenter translational study. J Med Dent. 2026;2(2):59–71.
[13] Yildirim A, Hertach R, Yildirim V. AI-assisted virtual surgical planning and 3D-printed splint transfer in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):72–84.
[14] Yildirim A, Hertach R, Yildirim V. Three-dimensional accuracy of AI-assisted virtual surgical planning in bimaxillary orthognathic surgery: a prospective comparative validation study. J Med Dent. 2026;2(2):85–98.
[15] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial comparing AI-assisted and conventional virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):99–110.
[16] Yildirim A, Hertach R, Yildirim V. Long-term skeletal stability and patient-reported outcomes following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):111–116.
[17] Yildirim A, Hertach R, Yildirim V. AI-assisted soft tissue prediction and facial symmetry analysis following bimaxillary orthognathic surgery: a prospective three-dimensional clinical study. J Med Dent. 2026;2(2):117–126.
[18] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of skeletal relapse and long-term stability following bimaxillary orthognathic surgery: a prospective three-dimensional analysis. J Med Dent. 2026;2(2):127–138.
[19] Yildirim A, Hertach R, Yildirim V. Multicenter external validation of AI-assisted virtual surgical planning in bimaxillary orthognathic surgery: a comparative Swiss-German clinical study. J Med Dent. 2026;2(2):139–149.
[20] Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56.
[21] Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial intelligence in surgery: promises and perils. Ann Surg. 2018;268(1):70–76.
[22] Maier-Hein L, Vedula SS, Speidel S, Navab N, Kikinis R, Park A, Eisenmann M, Feussner H, Forestier G, Giannarou S, et al. Surgical data science for next-generation interventions. Nat Biomed Eng. 2017;1:691–696.
[23] Arik SÖ, Ibragimov B, Xing L. Fully automated quantitative cephalometry using convolutional neural networks. J Med Imaging. 2017;4(1):014501.
[24] Hwang HW, Park JH, Moon JH, Yu Y, Kim H, Her SB, Srinivasan G, Aljanabi MNA, Donatelli RE, Lee SJ. Automated identification of cephalometric landmarks using deep learning. Angle Orthod. 2020;90(4):586–594.
[25] Kim H, Shim E, Park J, Kim YJ, Lee U, Kim Y. Web-based fully automated cephalometric analysis by deep learning. Comput Methods Programs Biomed. 2020;194:105513.