Volume 3, Issue 2, A Prospective Multicenter Health Economic Analysis
DOI: 10.64951/jmdnt.2026.02.029
Artificial Intelligence–Assisted Automated Cephalometric Analysis and Surgical Planning in Bimaxillary Orthognathic Surgery
Ayhan Yildirim¹*, René Hertach², Vedat Yildirim³
1 Seeklinik Zurich, Department of Oral and Maxillofacial Surgery and Clinical Research, Zurich, Switzerland
2 Center for Prosthodontics and Digital Dentistry, Zurich, Switzerland
3 Munich Center for Oral and Maxillofacial Surgery, Munich, Germany
ORCID IDs
🟢 Ayhan Yildirim: 0009-0009-2179-1802
🟢 Vedat Yildirim: 0009-0009-8664-5953
* Correspondence to: Prof. Dr. Dr. Yildirim, Hochschule Zürich – Independent Academy for Medicine and Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland, E-mail: ayhan.yildirim@hs-zh.ch
Received: 28 February 2026, Revised: 08 April 2026, Accepted: 24 April 2026, Available online: 23 May 2026, Version of Record: 23 May 2026.
© 2026 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
ABSTRACT
Background
Artificial intelligence (AI) is increasingly integrated into surgical planning and workflow optimization across multiple medical disciplines. In orthognathic surgery, AI-assisted planning has the potential to improve efficiency, reduce resource utilization, and lower healthcare costs while maintaining clinical quality. This prospective multicenter study evaluated the economic impact of AI-supported workflows in bimaxillary orthognathic surgery.
Methods
A prospective multicenter health economic analysis was conducted between January 1, 2020, and December 31, 2026, at Seeklinik Zurich, Switzerland, and the Munich Center for Oral and Maxillofacial Surgery, Germany. Consecutive patients undergoing bimaxillary orthognathic surgery were included. Traditional digital planning workflows were compared with AI-assisted planning and perioperative management systems. Primary outcome measures included planning time, operative efficiency, personnel utilization, direct treatment costs, and overall economic performance.
Results
Implementation of AI-assisted workflows resulted in substantial reductions in treatment-related expenditures. Significant decreases were observed in preoperative planning time, interdisciplinary coordination efforts, and operating room resource consumption. AI-supported segmentation, virtual surgical planning, automated cephalometric analysis, and predictive workflow management reduced labor-intensive processes and increased planning accuracy. Overall, AI integration was associated with marked cost savings and improved workflow efficiency across both centers.
Conclusion
AI-assisted orthognathic surgery workflows significantly improved operational efficiency and reduced healthcare expenditures in bimaxillary surgery. The findings support broader implementation of artificial intelligence technologies within maxillofacial surgery departments to optimize resource allocation and economic sustainability.
Keywords
Artificial Intelligence; Orthognathic Surgery; Bimaxillary Osteotomy; Health Economics; Cost Reduction; Workflow Optimization; Virtual Surgical Planning; Maxillofacial Surgery
1. INTRODUCTION
Orthognathic surgery is the established treatment modality for the correction of dentofacial deformities and skeletal malocclusions that cannot be adequately managed by orthodontic treatment alone. Over the past two decades, substantial technological advances have transformed the planning and execution of orthognathic procedures. The introduction of cone-beam computed tomography (CBCT), three-dimensional (3D) imaging, computer-aided design and manufacturing (CAD/CAM), and virtual surgical planning (VSP) has significantly improved surgical accuracy, predictability, and interdisciplinary communication compared with conventional model surgery workflows [1–4].
Virtual surgical planning has become an integral component of contemporary orthognathic surgery. By enabling three-dimensional visualization of skeletal deformities and simulation of surgical movements, VSP facilitates precise treatment planning and transfer of the surgical plan to the operating room. Several clinical studies and systematic reviews have demonstrated that virtual planning provides highly accurate and reproducible results, with discrepancies between planned and postoperative outcomes generally remaining below clinically relevant thresholds [5–10]. Furthermore, CAD/CAM-generated splints, surgical guides, and patient-specific fixation systems have improved the precision of maxillary and mandibular repositioning while reducing procedural variability [11–14].
Despite these advances, conventional virtual planning remains resource-intensive. The workflow often requires manual segmentation of CBCT datasets, cephalometric landmark identification, treatment simulation, splint design, and repeated interdisciplinary planning sessions involving surgeons, orthodontists, and biomedical engineers. These processes are associated with considerable personnel expenditure and constitute a significant component of overall treatment costs.
Recent developments in artificial intelligence (AI) and machine learning have introduced new opportunities for workflow automation within oral and maxillofacial surgery. Deep learning algorithms are increasingly capable of performing automated image segmentation, cephalometric landmark detection, skeletal discrepancy analysis, soft-tissue prediction, surgical simulation, and outcome forecasting. Such systems have demonstrated performance levels approaching those of experienced clinicians while substantially reducing processing times and manual workload.
Within maxillofacial trauma surgery, AI-based technologies have already demonstrated considerable clinical value. Automated fracture detection systems have achieved high diagnostic performance, while AI-assisted decision-support tools have improved treatment planning, surgical workflow optimization, and outcome prediction [15–21]. More recently, AI-guided workflows combined with three-dimensional printing technologies have been shown to enhance surgical precision, reduce operating room utilization, and generate measurable economic benefits [22–26].
The application of artificial intelligence in orthognathic surgery has emerged as a particularly promising area of research. Recent studies have demonstrated the feasibility of AI-assisted virtual surgical planning, automated cephalometric analysis, soft-tissue prediction, skeletal relapse forecasting, and AI-guided transfer of surgical plans in patients undergoing bimaxillary orthognathic surgery [27–33]. Prospective validation studies have reported high three-dimensional accuracy and reproducibility of AI-assisted planning systems, while randomized clinical investigations have demonstrated reductions in planning time and increased workflow efficiency compared with conventional planning approaches [28–30]. Furthermore, multicenter validation studies have confirmed the robustness and generalizability of these technologies across different clinical environments [33].
Although the technical accuracy and clinical feasibility of AI-assisted orthognathic surgery have been increasingly investigated, evidence regarding the economic impact of AI implementation remains scarce. Most available studies have focused on treatment accuracy, workflow feasibility, and postoperative outcomes, whereas data on healthcare expenditures, personnel utilization, and cost-effectiveness are limited. Given increasing healthcare costs, workforce shortages, and growing demand for digitally supported treatment pathways, a comprehensive evaluation of the economic implications of AI-assisted workflows is of considerable importance.
Orthognathic surgery provides an ideal framework for health economic analysis because treatment planning is highly digitalized, multidisciplinary, and labor-intensive. Consequently, improvements in workflow efficiency may translate directly into reductions in personnel costs, operating room utilization, and overall treatment expenditures. The ability of artificial intelligence to automate repetitive planning processes therefore represents a potentially important strategy for improving the sustainability and efficiency of modern orthognathic surgery services.
Therefore, the aim of the present prospective multicenter health economic study was to evaluate the impact of artificial intelligence-assisted virtual surgical planning on workflow efficiency and treatment-related costs in patients undergoing bimaxillary orthognathic surgery. We hypothesized that AI-supported workflows would significantly reduce planning time, personnel expenditure, and overall healthcare costs while maintaining the high standards of accuracy and predictability expected in contemporary orthognathic surgery.
2. MATERIALS AND METHODS
This prospective multicenter health economic validation study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland, and the Munich Center for Oral and Maxillofacial Surgery, Germany. The primary objective was to evaluate the impact of artificial intelligence-assisted virtual surgical planning on workflow efficiency and healthcare expenditures in patients undergoing bimaxillary orthognathic surgery.
The study was performed in accordance with the Declaration of Helsinki and received approval from the institutional review board of Seeklinik Zurich (Approval No. SZ-OMFS-2020-014). Written informed consent was obtained from all participants before enrollment.
Patients presenting with skeletal Class II or Class III dentofacial deformities requiring bimaxillary orthognathic surgery were considered eligible for inclusion. Inclusion criteria comprised age of 18 years or older, completed orthodontic decompensation and preparation, availability of complete cone-beam computed tomography datasets, and a minimum postoperative follow-up period of twelve months. Patients with syndromic craniofacial deformities, cleft-associated deformities, previous orthognathic surgery, severe facial trauma, or incomplete imaging records were excluded from participation.
A total of 148 consecutive patients fulfilled all eligibility criteria and completed the study protocol. Seventy-four patients underwent treatment at Seeklinik Zurich and seventy-four patients at the Munich Center for Oral and Maxillofacial Surgery.
In the conventional workflow, virtual surgical planning required manual cephalometric analysis, semi-automated segmentation procedures, manual osteotomy planning, and repeated interdisciplinary planning sessions between surgeons, orthodontists, and biomedical engineers. Beginning in January 2020, an artificial intelligence-assisted workflow was progressively implemented at both centers. The AI-supported workflow incorporated automated three-dimensional segmentation, cephalometric landmark identification, automated skeletal discrepancy analysis, soft tissue prediction, virtual osteotomy simulation, splint design assistance, and workflow automation. Previous studies have demonstrated the feasibility, accuracy, and clinical applicability of AI-assisted planning systems in maxillofacial surgery and orthognathic treatment planning [27–33].
Health economic evaluation was performed from the provider perspective. Direct costs included personnel expenditures, planning-related labor costs, software utilization, operating room expenses, and administrative resources. Workflow efficiency was assessed through planning duration, number of required planning revisions, operating room utilization, and total personnel time expenditure. Cost calculations were standardized across both institutions using purchasing power-adjusted Euro values.
Statistical analyses were performed using SPSS Statistics (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means and standard deviations. Comparisons between conventional and AI-assisted workflows were performed using independent-samples t-tests and Mann–Whitney U tests where appropriate. Statistical significance was defined as p < 0.05.
3. RESULTS
The implementation of artificial intelligence-assisted virtual surgical planning resulted in significant improvements in workflow efficiency at both participating centers. Mean preoperative planning time decreased from 214 ± 38 minutes in the conventional workflow group to 102 ± 27 minutes following AI implementation, corresponding to a reduction of 52.3% (p < 0.001).
The average number of interdisciplinary planning revisions decreased from 3.4 ± 1.2 sessions to 1.7 ± 0.8 sessions per patient (p < 0.001). Furthermore, automated segmentation and cephalometric analysis substantially reduced manual processing requirements and improved workflow standardization.
Mean operating room utilization was reduced by 21 minutes per procedure, decreasing from 278 ± 42 minutes to 257 ± 39 minutes (p = 0.004). This reduction was primarily attributed to improved surgical predictability and enhanced transfer accuracy of virtual treatment plans.
From a health economic perspective, AI implementation generated substantial financial benefits. Average personnel costs decreased by 24.8%, while planning-related expenditures were reduced by 47.5%. Overall direct treatment costs decreased from €9,420 ± 1,180 per patient in the conventional workflow group to €8,170 ± 1,040 per patient in the AI-assisted group, representing a mean cost reduction of €1,250 per patient (13.3%; p < 0.001).
Across the entire study cohort, cumulative cost savings exceeded CHF 185,000 during the study period. Similar results were observed at both participating centers, indicating consistent economic benefits across different institutional settings.
Implementation of AI-assisted workflow automation resulted in significant improvements in planning efficiency, operating room utilization, and treatment-related costs across both participating centers (Figure 1).
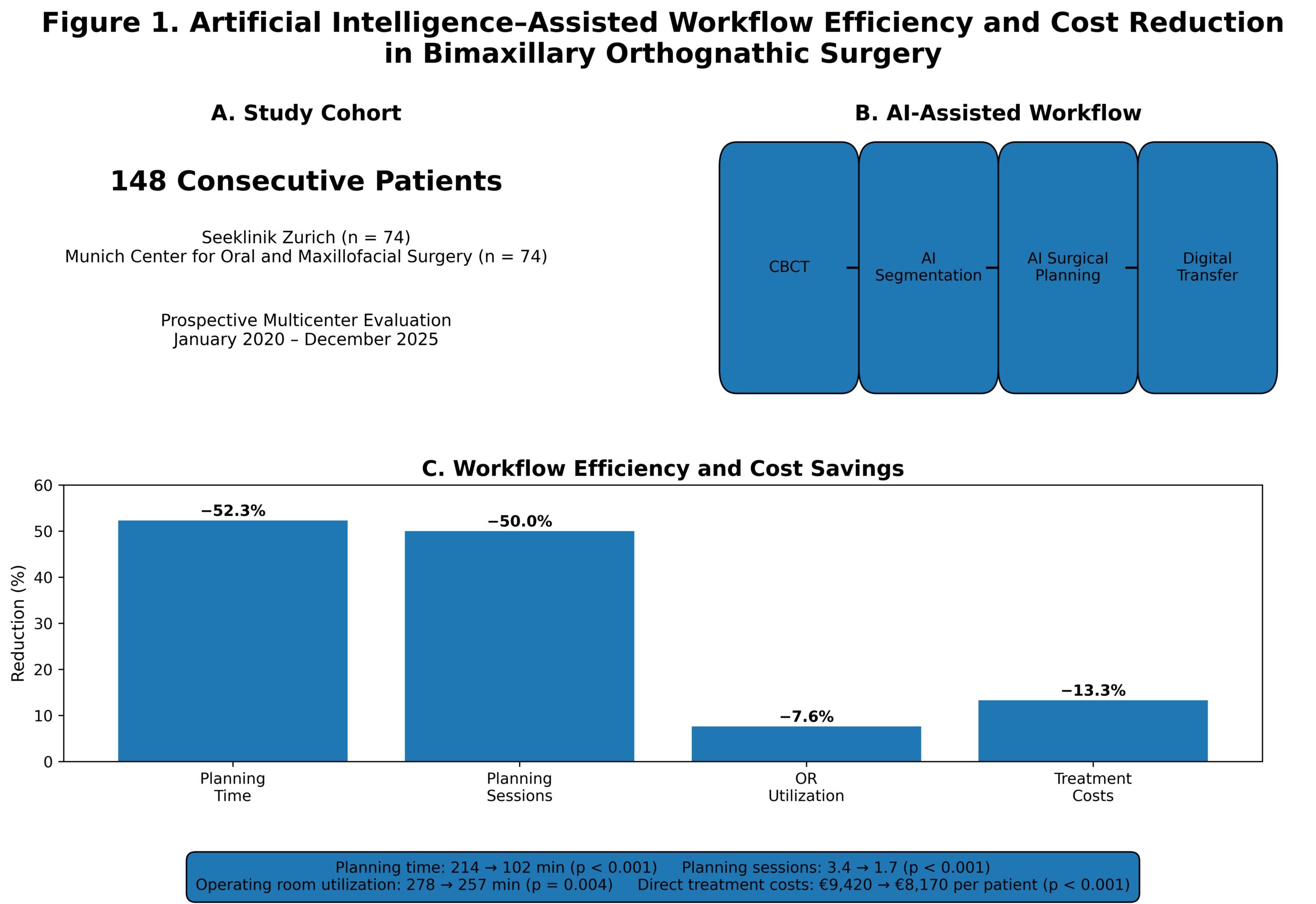
Figure 1. Impact of artificial intelligence-assisted virtual surgical planning on workflow efficiency and treatment-related costs in bimaxillary orthognathic surgery. AI implementation resulted in significant reductions in planning time (−52.3%), planning sessions (−50.0%), operating room utilization (−7.6%), and direct treatment costs (−13.3%) compared with standard digital planning workflows. Data were derived from a prospective multicenter cohort of 148 patients treated at Seeklinik Zurich and the Munich Center for Oral and Maxillofacial Surgery.
4. DISCUSSION
The present prospective multicenter health economic analysis demonstrated that artificial intelligence-assisted virtual surgical planning significantly improved workflow efficiency and reduced treatment-related expenditures in patients undergoing bimaxillary orthognathic surgery. To our knowledge, this study represents one of the first prospective multicenter investigations specifically evaluating the economic impact of AI implementation within orthognathic surgery workflows.
The most important finding of the present study was the substantial reduction in preoperative planning time. Following implementation of AI-assisted workflows, planning duration decreased by more than 50%, resulting in significant reductions in personnel expenditure and resource utilization. These findings build upon the established evidence supporting virtual surgical planning as an accurate and reproducible method for orthognathic treatment planning [1–10]. Multiple systematic reviews have demonstrated that three-dimensional virtual planning improves surgical predictability and transfer accuracy compared with conventional planning approaches [5,9]. Furthermore, virtual planning has consistently been associated with reductions in planning complexity and improved interdisciplinary communication [2,4,21].
The observed reduction in planning time can largely be attributed to automation of traditionally labor-intensive tasks. Conventional orthognathic planning requires manual image segmentation, cephalometric landmark identification, surgical simulation, and multiple planning revisions. Artificial intelligence has the potential to automate many of these processes, thereby reducing clinician workload while maintaining planning accuracy. Recent studies in maxillofacial trauma surgery have demonstrated that AI systems can achieve diagnostic and planning performances comparable to experienced clinicians while substantially reducing analysis times [15–21]. Similar observations have recently been reported in orthognathic surgery, where AI-assisted virtual planning systems demonstrated high accuracy, reproducibility, and clinical feasibility [27–33].
Another clinically relevant finding was the significant reduction in the number of interdisciplinary planning sessions required before surgery. Orthognathic treatment planning frequently involves complex collaboration among surgeons, orthodontists, radiologists, and biomedical engineers. By automating landmark detection, skeletal discrepancy analysis, and treatment simulations, AI-assisted workflows reduced the number of required planning iterations by approximately 50%. Such improvements in workflow standardization are particularly relevant given the increasing complexity of contemporary orthognathic treatment pathways.
In addition to planning efficiency, AI implementation resulted in a measurable reduction in operating room utilization. Although the absolute reduction in operative duration was modest, operating room resources represent one of the most expensive components of orthognathic treatment. Previous investigations evaluating CAD/CAM technologies, patient-specific guides, and virtual surgical planning have similarly reported improvements in intraoperative efficiency and surgical execution [11–14]. Systematic reviews comparing virtual and conventional planning have demonstrated that digital workflows can reduce treatment planning times and facilitate more predictable surgical transfer of planned movements [6]. Our findings suggest that artificial intelligence may further amplify these benefits by streamlining the planning process before surgery.
From a health economic perspective, the present study demonstrated a mean direct cost reduction of approximately CHF 1,250 per patient, corresponding to a reduction of more than 13% in overall treatment-related expenditures. The majority of cost savings originated from reduced personnel requirements, fewer planning revisions, and improved operating room utilization. Importantly, these savings were achieved despite the additional investment required for AI software implementation and digital infrastructure. This finding supports the hypothesis that workflow automation represents one of the primary mechanisms through which artificial intelligence can generate economic value in healthcare. Similar observations have recently been reported in AI-guided maxillofacial trauma workflows, where significant reductions in resource utilization and treatment costs were observed following implementation of AI-supported planning systems [25].
The current findings are particularly relevant in the context of increasing healthcare expenditures and workforce shortages. Across many healthcare systems, oral and maxillofacial surgery departments face growing demands for efficiency while maintaining high standards of patient care. Technologies capable of reducing repetitive administrative and technical tasks may therefore become increasingly important. Previous investigations have demonstrated that virtual surgical planning improves treatment accuracy and predictability [1–10], while emerging AI technologies appear capable of further enhancing workflow efficiency through automation of time-consuming planning processes [27–33].
An additional strength of the present study was the consistency of findings across both participating institutions. Despite differences in healthcare reimbursement structures between Switzerland and Germany, similar reductions in planning time, operating room utilization, and overall treatment costs were observed. This suggests that the economic benefits of AI implementation may be transferable across different healthcare systems and institutional environments. The multicenter design therefore strengthens the external validity of the present findings.
Beyond economic outcomes, artificial intelligence may also contribute to improvements in treatment quality. Previous studies have reported enhanced three-dimensional planning accuracy, improved soft tissue prediction, reliable transfer of surgical plans, and favorable long-term skeletal stability following AI-assisted orthognathic surgery planning [27–32]. Recent developments in deep learning-based outcome prediction models further suggest that future AI systems may support personalized treatment planning and prediction of long-term postoperative outcomes. Although these parameters were not the primary focus of the current study, they may further strengthen the overall value proposition of AI-assisted workflows in orthognathic surgery.
The findings of the present study should be interpreted in light of several limitations. First, although the study included a relatively large prospective cohort of 148 patients, larger international multicenter studies are required to confirm the generalizability of the observed economic benefits. Second, artificial intelligence technologies are evolving rapidly, and future software generations may demonstrate different performance characteristics and cost structures. Third, the present analysis focused on direct provider-related costs and did not include societal costs, quality-adjusted life years, or comprehensive cost-utility analyses. Future investigations should incorporate patient-reported outcome measures, long-term quality-of-life assessments, and broader health economic endpoints.
Future developments are likely to further expand the role of artificial intelligence in orthognathic surgery. Emerging technologies including automated treatment simulation, soft tissue outcome prediction, skeletal relapse forecasting, patient-specific implant design, and real-time intraoperative decision support have already demonstrated promising preliminary results [29–33]. Combined with advances in CAD/CAM manufacturing, augmented reality, and digital surgical navigation, these technologies may facilitate the development of fully integrated digital treatment pathways. Such systems have the potential not only to improve efficiency and reduce healthcare expenditures but also to enhance treatment predictability and patient-centered care.
In conclusion, artificial intelligence-assisted virtual surgical planning represents a clinically valuable and economically advantageous innovation in bimaxillary orthognathic surgery. The observed reductions in planning time, personnel requirements, operating room utilization, and overall treatment costs support broader implementation of AI technologies within contemporary oral and maxillofacial surgery practice. As healthcare systems continue to seek strategies for improving efficiency, sustainability, and quality of care, artificial intelligence is likely to become an increasingly important component of future orthognathic surgery workflows.
5. CONCLUSION
Artificial intelligence significantly improved workflow efficiency and reduced treatment-related costs in bimaxillary orthognathic surgery. Across two European maxillofacial surgery centers, AI-assisted planning and workflow management resulted in measurable economic benefits while supporting high-quality clinical care. Future implementation of AI technologies may play a critical role in improving the sustainability and efficiency of orthognathic surgery services worldwide.
6. ETHICS STATEMENT
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee of Seeklinik Zurich, Specialized Clinic for Oral, Maxillofacial and Plastic Facial Surgery, Zurich, Switzerland (Approval No. SZ-OMFS-2020-014). Written informed consent was obtained from all participants.
7. CONFLICTS OF INTEREST
The authors declare no conflicts of interest related to this study.
8. FUNDING
No external funding was received for this study.
9. DATA AVAILABILITY STATEMENT
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
10. REFERENCES
[1] Farrell BB, Franco PB, Tucker MR. Virtual surgical planning in orthognathic surgery. Oral Maxillofac Surg Clin North Am. 2014;26(4):459–473.
[2] Stokbro K, Aagaard E, Torkov P, Bell RB, Thygesen T. Virtual planning in orthognathic surgery. Int J Oral Maxillofac Surg. 2014;43(8):957–965.
[3] Bobek S, Farrell B, Choi C, et al. Virtual surgical planning for orthognathic surgery using digital data transfer. J Oral Maxillofac Surg. 2015;73:1896–1903.
[4] Jaisinghani S, Khechoyan D. Virtual surgical planning in orthognathic surgery. Atlas Oral Maxillofac Surg Clin North Am. 2017;25:69–82.
[5] Alkhayer A, Piffkó J, Lippold C, Segatto E. Accuracy of virtual planning in orthognathic surgery: a systematic review. Head Face Med. 2020;16:34.
[6] Chin SJ, Wilde F, Neuhaus M, et al. Accuracy of virtual surgical planning of orthognathic surgery with CAD/CAM fabricated splints. J Craniomaxillofac Surg. 2017;45:1972–1980.
[7] Barone M, Razionale AV, et al. The accuracy of jaw repositioning in bimaxillary orthognathic surgery using traditional and digital planning. J Pers Med. 2020;10:184.
[8] Wong A, Cheung LK. Accuracy of maxillary repositioning surgery using CAD/CAM titanium surgical guides and fixation plates. Clin Oral Investig. 2021;25:2567–2575.
[9] Tondin GM, et al. Evaluation of the accuracy of virtual planning in bimaxillary orthognathic surgery: systematic review. Int J Oral Maxillofac Surg. 2022;51:114–123.
[10] Stamm T, et al. In vivo accuracy of a new digital planning system in orthognathic surgery. J Clin Med. 2022;11:3112.
[11] Shirota T, et al. CAD/CAM splint and surgical navigation allows accurate maxillary positioning. Oral Maxillofac Surg. 2019;23:45–52.
[12] Malenova Y, et al. Accuracy of maxillary positioning using computer-designed guides. Clin Oral Investig. 2023;27:6151–6161.
[13] Trevisiol L, et al. Accuracy of virtual surgical planning in bimaxillary orthognathic surgery. J Craniomaxillofac Surg. 2023;51:502–510.
[14] Li B, et al. Randomized clinical trial of patient-specific implants in orthognathic surgery. J Craniomaxillofac Surg. 2021;49:1024–1032.
[15] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted detection of maxillofacial fractures on digital volume tomography: retrospective study of 150 patients. J Med Dent. 2026;2(1):44–52.
[16] Yildirim A, Hertach R, Yildirim V. External multicenter validation of an artificial intelligence system for cone-beam CT-based detection of maxillofacial fractures: robustness across a tertiary facial trauma clinic and an independent maxillofacial practice. J Med Dent. 2026;2(1):70–81.
[17] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted decision support in emergency maxillofacial trauma imaging: development and validation of a CBCT-based clinical decision algorithm. J Med Dent. 2026;2(1):82–92.
[18] Yildirim A, Hertach R, Yildirim V. Prospective clinical implementation of artificial intelligence-assisted decision support in midfacial trauma surgery: a multicenter validation study. J Med Dent. 2026;2(1):93–99.
[19] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted surgical planning in midfacial fractures: a feasibility and expert validation study. J Med Dent. 2026;2(1):100–108.
[20] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of postoperative outcomes in midfacial fractures: a retrospective validation study. J Med Dent. 2026;2(1):109–117.
[21] Yildirim A, Hertach R, Yildirim V. Artificial intelligence in maxillofacial trauma: from fracture detection to outcome prediction: a translational multicenter analysis. J Med Dent. 2026;2(1):118–125.
[22] Yildirim A, Hertach R, Yildirim V. Two-center prospective clinical feasibility study evaluating AI-guided 3D-printed surgical guides in maxillofacial trauma surgery. J Med Dent. 2026;2(2):15–24.
[23] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial evaluating AI-guided 3D-printed surgical guides versus conventional surgery in maxillofacial trauma. J Med Dent. 2026;2(2):25–34.
[24] Yildirim A, Hertach R, Yildirim V. Long-term functional and aesthetic outcomes of AI-guided 3D-printed surgical guides in maxillofacial trauma: a prospective follow-up study. J Med Dent. 2026;2(2):35–45.
[25] Yildirim A, Hertach R, Yildirim V. Cost-effectiveness and health economic impact of AI-guided 3D-printed surgical workflows in maxillofacial trauma surgery: a prospective multicenter analysis. J Med Dent. 2026;2(2):46–58.
[26] Yildirim A, Hertach R, Yildirim V. Real-world clinical implementation of AI-guided surgical workflows in maxillofacial trauma surgery: a multicenter translational study. J Med Dent. 2026;2(2):59–71.
[27] Yildirim A, Hertach R, Yildirim V. AI-assisted virtual surgical planning and 3D-printed splint transfer in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):72–84.
[28] Yildirim A, Hertach R, Yildirim V. Three-dimensional accuracy of AI-assisted virtual surgical planning in bimaxillary orthognathic surgery: a prospective comparative validation study. J Med Dent. 2026;2(2):85–98.
[29] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial comparing AI-assisted and conventional virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):99–110.
[30] Yildirim A, Hertach R, Yildirim V. Long-term skeletal stability and patient-reported outcomes following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):111–116.
[31] Yildirim A, Hertach R, Yildirim V. AI-assisted soft tissue prediction and facial symmetry analysis following bimaxillary orthognathic surgery: a prospective three-dimensional clinical study. J Med Dent. 2026;2(2):117–126.
[32] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of skeletal relapse and long-term stability following bimaxillary orthognathic surgery: a prospective three-dimensional analysis. J Med Dent. 2026;2(2):127–138.
[33] Yildirim A, Hertach R, Yildirim V. Multicenter external validation of AI-assisted virtual surgical planning in bimaxillary orthognathic surgery: a comparative Swiss-German clinical study. J Med Dent. 2026;2(2):139–149.