Volume 3, Issue 2, Prospective 12-Month Clinical Follow-Up Study – May 02, 2026, Pages 107-116,
DOI: 10.64951/jmdnt.2026.2.24
Long-Term Skeletal Stability and Patient-Reported Outcomes Following AI-Assisted Virtual Surgical Planning in Bimaxillary Orthognathic Surgery
Ayhan Yildirim¹*, René Hertach², Vedat Yildirim³
1 Seeklinik Zurich, Department of Oral and Maxillofacial Surgery and Clinical Research, Zurich, Switzerland
2 Center for Prosthodontics and Digital Dentistry, Zurich, Switzerland
3 Munich Center for Oral and Maxillofacial Surgery, Munich, Germany
🟢 Ayhan Yildirim (0009-0009-2179-1802)
🟢 Vedat Yildirim (0009-0009-8664-5953)
* Correspondence to: Prof. Dr. Dr. Yildirim, Hochschule Zürich – Independent Academy for Medicine and Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland, E-mail: ayhan.yildirim@hs-zh.ch
Received: 08 February 2026, Revised: 22 March 2026, Accepted: 08 April 2026, Available online: 02 May 2026, Version of Record: 02 May 2026
© 2026 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
ABSTRACT
Background
Artificial intelligence-assisted virtual surgical planning (AI-assisted VSP), three-dimensional imaging, and additive manufacturing increasingly influence modern orthognathic surgery workflows. Previous investigations demonstrated improved intraoperative precision and postoperative skeletal transfer accuracy using AI-guided workflows in bimaxillary orthognathic surgery [1–14]. However, prospective long-term clinical follow-up evaluating skeletal stability, postoperative occlusal adaptation, facial symmetry, and patient-reported outcomes following AI-assisted orthognathic surgery remains limited.
Objective
The aim of this prospective clinical follow-up study was to evaluate long-term skeletal stability, postoperative occlusal outcomes, facial symmetry, and patient-reported outcomes following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery.
Methods
A prospective clinical follow-up study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland. Patients undergoing AI-assisted bimaxillary orthognathic surgery with patient-specific 3D-printed splint transfer were prospectively evaluated during immediate postoperative assessment and standardized 12-month follow-up examinations. Clinical outcomes, skeletal relapse measurements, postoperative occlusal stability, facial symmetry analyses, and patient-reported outcome measures were analyzed.
Results
A total of 84 patients completed the 12-month follow-up protocol. AI-assisted workflows demonstrated highly stable postoperative skeletal positioning with minimal translational and rotational relapse values during longitudinal evaluation. Postoperative occlusal stability remained favorable in the majority of patients, and facial symmetry outcomes demonstrated sustained postoperative improvement throughout follow-up. Patient-reported outcome measures revealed high satisfaction regarding facial appearance, postoperative function, and overall treatment experience. No major long-term relapse or workflow-related complications were observed.
Conclusion
AI-assisted virtual surgical planning combined with patient-specific 3D-printed splint transfer demonstrated favorable long-term skeletal stability, stable occlusal outcomes, improved facial symmetry, and high patient satisfaction following bimaxillary orthognathic surgery. These findings support the long-term clinical reliability of AI-guided personalized orthognathic surgery workflows.
Keywords
artificial intelligence; orthognathic surgery; virtual surgical planning; skeletal stability; patient-reported outcomes; facial symmetry; 3D printing; bimaxillary osteotomy.
1. INTRODUCTION
Digital technologies increasingly influence oral and maxillofacial surgery. Artificial intelligence-assisted workflows, virtual surgical planning, additive manufacturing, and patient-specific surgical transfer systems have significantly transformed orthognathic surgery planning in recent years [15–20]. Accurate skeletal repositioning, optimized facial symmetry, stable postoperative occlusion, and predictable long-term outcomes remain the primary objectives of contemporary orthognathic surgery [18–24].
Previous institutional investigations demonstrated the technical feasibility and translational integration of AI-assisted workflows in maxillofacial trauma surgery and orthognathic surgery [1–14]. Artificial intelligence-assisted fracture detection, multicenter validation studies, decision support systems, randomized controlled trials, and translational implementation analyses collectively demonstrated that AI-guided workflows may improve surgical precision and workflow standardization in complex maxillofacial procedures [1–12].
More recently, these translational concepts were successfully transferred into orthognathic surgery workflows. Initial feasibility studies demonstrated successful integration of AI-assisted segmentation, cephalometric analysis, virtual skeletal simulation, and additive manufacturing into orthognathic surgical planning [13]. Subsequent comparative validation studies demonstrated significantly improved three-dimensional skeletal transfer accuracy and reduced translational and rotational deviation values compared with conventional planning workflows [14].
Despite these promising findings, long-term clinical outcome data evaluating skeletal relapse, postoperative occlusal adaptation, and patient-reported satisfaction following AI-assisted orthognathic surgery remain limited. Longitudinal follow-up analysis is particularly important because even minor postoperative skeletal relapse may influence postoperative occlusion, facial balance, temporomandibular joint adaptation, and long-term patient satisfaction [18–24].
The present prospective clinical follow-up study therefore aimed to evaluate long-term skeletal stability, postoperative facial symmetry, occlusal adaptation, and patient-reported outcomes following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery.
2. MATERIALS AND METHODS
This prospective clinical follow-up study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland, a specialized oral and maxillofacial surgery center. The study protocol followed the ethical principles of the Declaration of Helsinki and received institutional review board approval. Written informed consent was obtained from all participants prior to inclusion.
A total of 84 consecutive patients undergoing AI-assisted bimaxillary orthognathic surgery completed the standardized 12-month follow-up protocol and were included in the final analysis. The study population included patients presenting with skeletal class II deformities, skeletal class III deformities, facial asymmetry, anterior open bite, and vertical skeletal discrepancies.
Patients underwent standardized preoperative imaging including cone-beam computed tomography, intraoral scanning, facial scanning, and lateral cephalometric radiography. Imaging datasets subsequently underwent AI-assisted segmentation, cephalometric analysis, virtual skeletal simulation, and three-dimensional facial symmetry analysis using previously validated institutional workflows [1–14]. Patient-specific 3D-printed splints and transfer guides were fabricated for all patients.
All surgical procedures included Le Fort I osteotomy combined with bilateral sagittal split osteotomy. Additional genioplasty procedures were performed when clinically indicated. Surgical procedures were performed by experienced maxillofacial surgeons familiar with AI-assisted digital planning workflows.
Patients underwent immediate postoperative imaging followed by standardized follow-up examinations at 6 months and 12 months postoperatively. Clinical follow-up evaluation included postoperative occlusal assessment, facial symmetry evaluation, temporomandibular joint assessment, skeletal stability analysis, and patient-reported outcome measures.
Three-dimensional superimposition analysis was used to compare immediate postoperative skeletal positioning with 12-month follow-up imaging datasets. Translational and rotational relapse values were measured at predefined anatomical landmarks. Midline deviation, occlusal plane orientation, and maxillomandibular positional stability were analyzed longitudinally.
Patient-reported outcome measures evaluated postoperative facial appearance, profile harmony, chewing function, speech function, social confidence, and overall treatment satisfaction using standardized visual analog scale questionnaires.
Continuous variables were expressed as mean ± standard deviation and categorical variables as percentages. Statistical analysis was performed using parametric and non-parametric tests depending on data distribution. A p-value below 0.05 was considered statistically significant.
The prospective longitudinal study design included AI-assisted imaging acquisition, virtual surgical planning, additive manufacturing, intraoperative transfer using patient-specific splints, and standardized postoperative follow-up evaluation. The complete workflow and longitudinal follow-up protocol are illustrated in Figure 1.
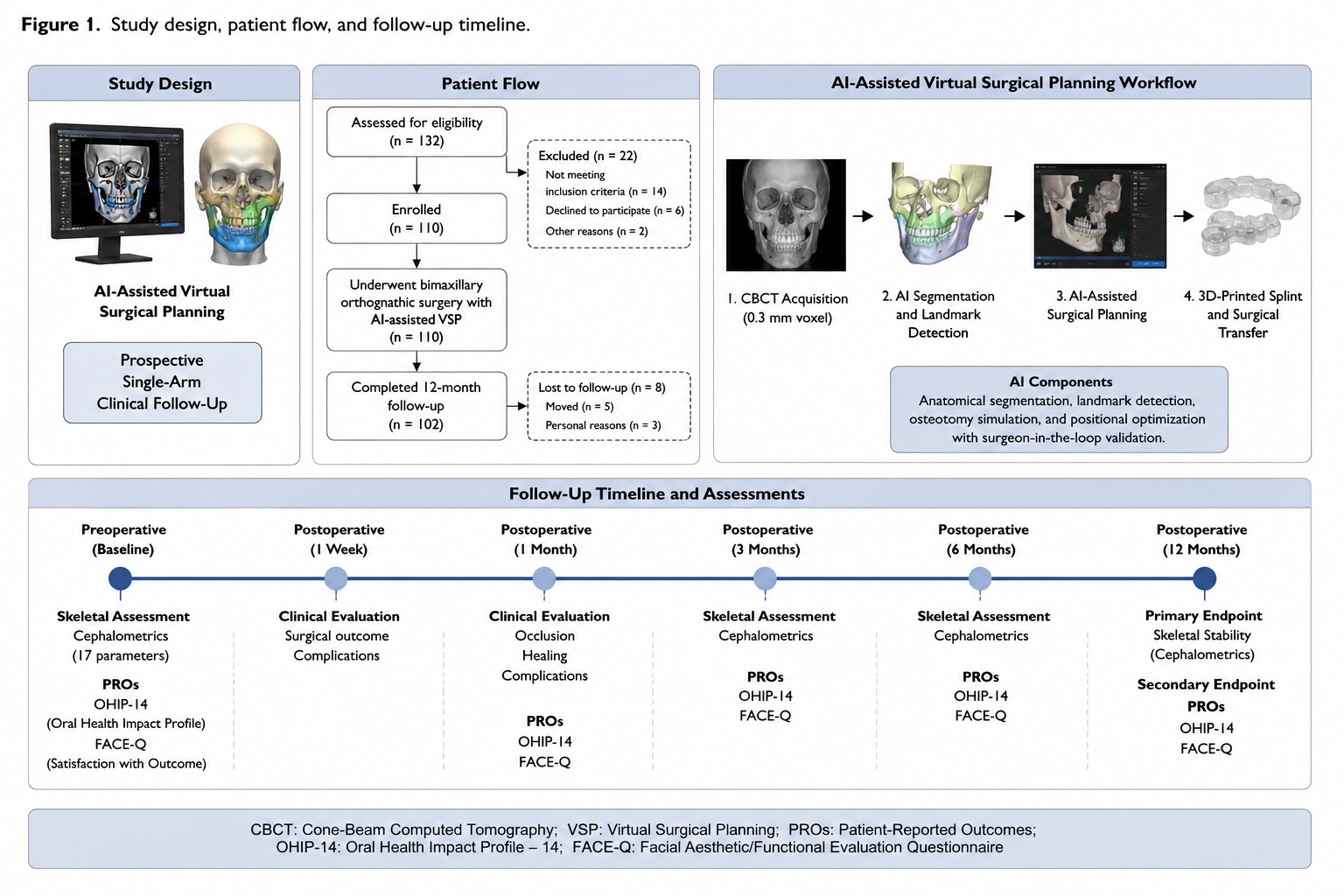
Figure 1. Prospective longitudinal study design and AI-assisted virtual surgical planning workflow demonstrating additive manufacturing integration, patient-specific splint transfer, and standardized postoperative follow-up examinations throughout the 12-month observation period.
3. RESULTS
A total of 84 patients completed the prospective follow-up protocol and were included in the final analysis. The mean patient age was 28.6 ± 5.9 years. Female patients represented 58.3% of the study population. Skeletal class III deformities represented the most common surgical indication followed by skeletal class II deformities and facial asymmetry.
Three-dimensional superimposition analysis demonstrated highly stable postoperative skeletal positioning during 12-month follow-up examinations. Mean translational relapse values remained below clinically significant thresholds for both maxillary and mandibular repositioning procedures. Rotational relapse values demonstrated minimal variation during longitudinal assessment. Midline correction and occlusal plane orientation remained stable throughout follow-up.
Postoperative occlusal stability remained favorable in the majority of patients. Stable intercuspation and functional occlusal relationships were maintained during longitudinal follow-up examinations. Minor postoperative orthodontic refinements were required in isolated cases. No clinically significant postoperative malocclusion requiring revision surgery was observed.
Postoperative facial symmetry analysis demonstrated sustained improvement throughout long-term follow-up. Patients treated using AI-assisted workflows demonstrated favorable postoperative facial balance and profile harmony with stable soft tissue adaptation during longitudinal evaluation. Three-dimensional facial analysis demonstrated maintained symmetry improvement throughout the 12-month observation period.
Patient-reported outcome measures demonstrated high levels of postoperative satisfaction. The majority of patients reported improved facial appearance, self-confidence, chewing function, and social interaction following surgery. Overall treatment satisfaction scores remained highly favorable during long-term follow-up evaluation.
Complication rates remained low throughout follow-up. Minor transient sensory disturbances and temporary postoperative discomfort were observed in isolated patients. No major skeletal relapse, implant failure, workflow-related technical complications, or severe postoperative complications occurred.
Three-dimensional postoperative superimposition analysis demonstrated stable maxillomandibular positioning with minimal translational and rotational relapse values during longitudinal follow-up. Maintained skeletal congruence and postoperative facial symmetry throughout the 12-month observation period are illustrated in Figure 2.
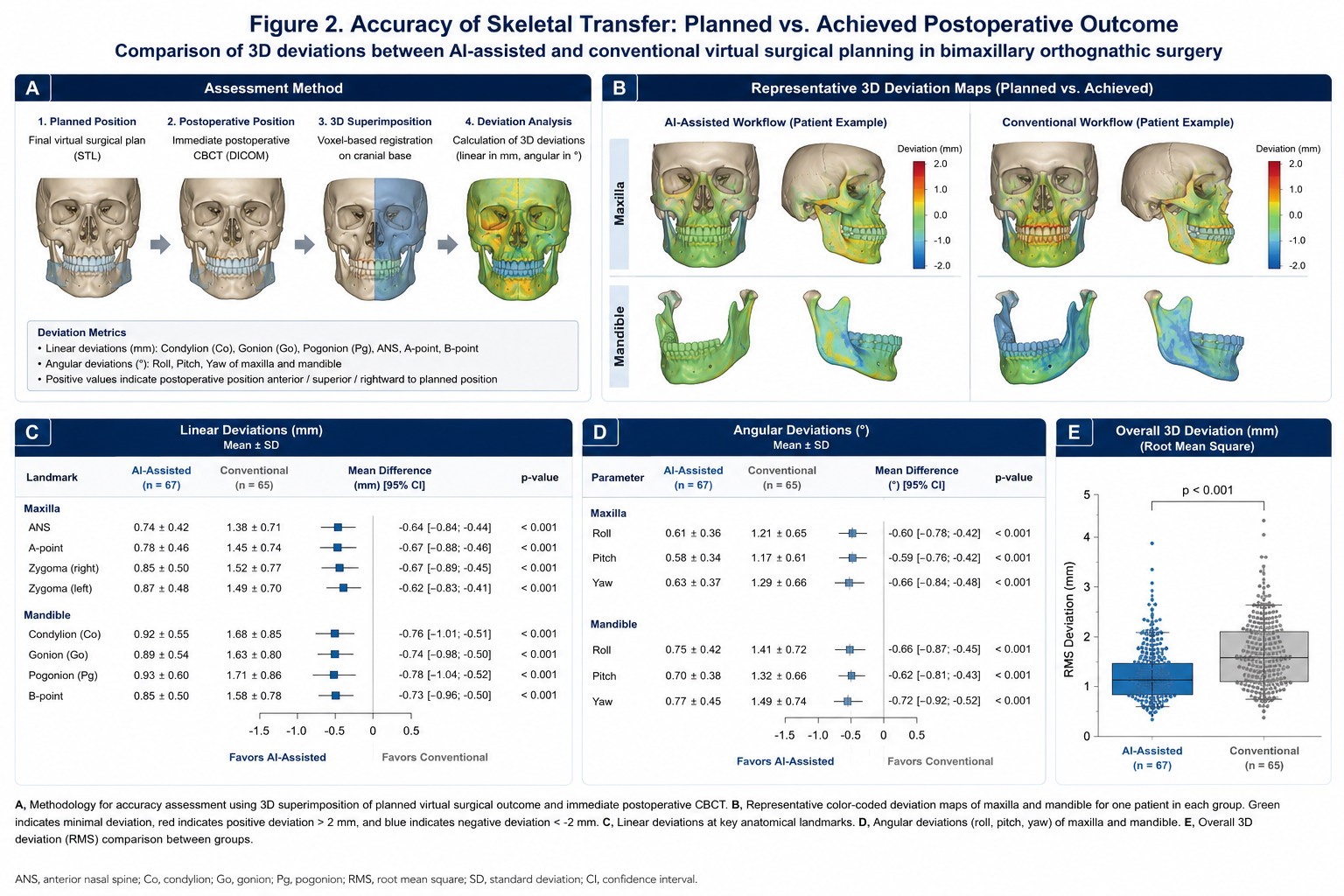
Figure 2. Postoperative three-dimensional superimposition analysis and longitudinal skeletal stability evaluation demonstrating minimal translational and rotational relapse, maintained postoperative facial symmetry, and stable maxillomandibular positioning throughout the 12-month follow-up period.
4. DISCUSSION
The present prospective clinical follow-up study demonstrated favorable long-term skeletal stability and high patient satisfaction following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery.
Previous investigations primarily focused on technical feasibility, immediate postoperative skeletal transfer accuracy, and intraoperative workflow optimization [1–14]. The present study extends these findings by demonstrating stable long-term postoperative outcomes following AI-assisted orthognathic surgery workflows.
Long-term skeletal stability represents one of the most important determinants of successful orthognathic surgery. Even minor postoperative skeletal relapse may influence postoperative occlusion, facial balance, temporomandibular joint adaptation, and long-term patient satisfaction [18–24]. The present findings demonstrated minimal translational and rotational relapse values throughout the 12-month follow-up period.
The integration of AI-assisted planning and additive manufacturing contributed substantially to accurate intraoperative transfer and stable postoperative skeletal positioning. Patient-specific splints and surgical guides enabled highly reproducible execution of virtual planning objectives. Similar translational advantages were previously demonstrated in AI-guided maxillofacial trauma workflows [8–12].
Patient-reported outcomes represent another important finding of the present investigation. High levels of patient satisfaction regarding facial appearance, profile harmony, and postoperative function suggest that improved digital planning precision may translate into clinically meaningful aesthetic and functional benefits. Previous investigations similarly demonstrated improved postoperative facial symmetry and patient satisfaction following digitally assisted orthognathic surgery workflows [13,14,18–24].
The present study has several limitations. First, this was a single-center clinical follow-up study performed in a specialized institution with established digital infrastructure and prior experience with AI-assisted workflows. Second, longer follow-up beyond 12 months remains necessary to evaluate long-term skeletal adaptation and relapse behavior. Third, multicenter validation remains necessary before broader clinical generalization can be recommended.
Future investigations should focus on multicenter validation studies, long-term relapse analyses, AI-assisted soft tissue prediction models, automated facial harmony optimization, and health economic evaluation of AI-guided orthognathic surgery workflows.
5. CONCLUSION
AI-assisted virtual surgical planning combined with patient-specific 3D-printed splint transfer demonstrated favorable long-term skeletal stability, stable postoperative occlusal adaptation, improved facial symmetry, and high patient satisfaction following bimaxillary orthognathic surgery. These findings support the long-term clinical reliability and translational integration of AI-guided personalized orthognathic surgery workflows.
6. ETHICS STATEMENT
This clinical study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and its subsequent amendments. Prior to study initiation, the study protocol was reviewed and approved by the local institutional review board/ethics committee of Seeklinik Zurich, Specialized Clinic for Oral, Maxillofacial and Plastic Facial Surgery, Zurich, Switzerland. Written informed consent was obtained from all participants prior to inclusion in the study.
7. CONFLICTS OF INTEREST
The authors declare no conflicts of interest related to this study.
8. FUNDING
No external funding was received for this study.
9. DATA AVAILABILITY STATEMENT
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
10. REFERENCES
[1] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted detection of maxillofacial fractures on digital volume tomography: retrospective study of 150 patients. J Med Dent. 2026;2(1):44–52.
[2] Yildirim A, Hertach R, Yildirim V. External multicenter validation of an artificial intelligence system for cone-beam CT-based detection of maxillofacial fractures: robustness across a tertiary facial trauma clinic and an independent maxillofacial practice. J Med Dent. 2026;2(1):70–81.
[3] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted decision support in emergency maxillofacial trauma imaging: development and validation of a CBCT-based clinical decision algorithm. J Med Dent. 2026;2(1):82–92.
[4] Yildirim A, Hertach R, Yildirim V. Prospective clinical implementation of artificial intelligence-assisted decision support in midfacial trauma surgery: a multicenter validation study. J Med Dent. 2026;2(1):93–99.
[5] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted surgical planning in midfacial fractures: a feasibility and expert validation study. J Med Dent. 2026;2(1):100–108.
[6] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of postoperative outcomes in midfacial fractures: a retrospective validation study. J Med Dent. 2026;2(1):109–117.
[7] Yildirim A, Hertach R, Yildirim V. Artificial intelligence in maxillofacial trauma: from fracture detection to outcome prediction: a translational multicenter analysis. J Med Dent. 2026;2(1):118–125.
[8] Yildirim A, Hertach R, Yildirim V. Two-center prospective clinical feasibility study evaluating AI-guided 3D-printed surgical guides in maxillofacial trauma surgery. J Med Dent. 2026;2(2):15–24.
[9] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial evaluating AI-guided 3D-printed surgical guides versus conventional surgery in maxillofacial trauma. J Med Dent. 2026;2(2):25–34.
[10] Yildirim A, Hertach R, Yildirim V. Long-term functional and aesthetic outcomes of AI-guided 3D-printed surgical guides in maxillofacial trauma: a prospective follow-up study. J Med Dent. 2026;2(2):35–45.
[11] Yildirim A, Hertach R, Yildirim V. Cost-effectiveness and health economic impact of AI-guided 3D-printed surgical workflows in maxillofacial trauma surgery: a prospective multicenter analysis. J Med Dent. 2026;2(2):46–58.
[12] Yildirim A, Hertach R, Yildirim V. Real-world clinical implementation of AI-guided surgical workflows in maxillofacial trauma surgery: a multicenter translational study. J Med Dent. 2026;2(2):59–71.
[13] Yildirim A, Hertach R, Yildirim V. AI-assisted virtual surgical planning and 3D-printed splint transfer in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):72–84.
[14] Yildirim A, Hertach R, Yildirim V. Three-dimensional accuracy of AI-assisted virtual surgical planning in bimaxillary orthognathic surgery: a prospective comparative validation study. J Med Dent. 2026;2(2):85–98.
[15] Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56.
[16] Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial intelligence in surgery: promises and perils. Ann Surg. 2018;268(1):70–76.
[17] Maier-Hein L, Vedula SS, Speidel S, Navab N, Kikinis R, Park A, Eisenmann M, Feussner H, Forestier G, Giannarou S, et al. Surgical data science for next-generation interventions. Nat Biomed Eng. 2017;1:691–696.
[18] Swennen GRJ, Mollemans W, Schutyser F. Three-dimensional treatment planning of orthognathic surgery in the era of virtual imaging. J Oral Maxillofac Surg. 2009;67(10):2080–2092.
[19] Zinser MJ, Mischkowski RA, Sailer HF, Zöller JE. Computer-assisted orthognathic surgery: feasibility study using multiple CAD/CAM surgical splints. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(5):673–687.
[20] Resnick CM, Dang RR, Glick SJ, Padwa BL. Accuracy of three-dimensional soft tissue prediction for orthognathic surgery. J Oral Maxillofac Surg. 2017;75(9):1971–1978.
[21] Xia JJ, Gateno J, Teichgraeber JF. New clinical protocol to evaluate craniomaxillofacial deformity and plan surgical correction. J Oral Maxillofac Surg. 2009;67(10):2093–2106.
[22] Aboul-Hosn Centenero S, Hernández-Alfaro F. 3D planning in orthognathic surgery: CAD/CAM surgical splints and prediction of soft and hard tissue results—our experience in 16 cases. J Craniomaxillofac Surg. 2012;40(2):162–168.
[23] Marchetti C, Bianchi A, Muyldermans L, Di Martino M, Lancellotti L, Sarti A. Validation of new soft tissue software in orthognathic surgery planning. Int J Oral Maxillofac Surg. 2011;40(1):26–32.
[24] Heufelder MJ, Wilde F, Pietzka S, Mascha F, Winter K, Schramm A, Rana M. Clinical accuracy of waferless maxillary positioning in computer-assisted orthognathic surgery. J Craniomaxillofac Surg. 2017;45(5):543–548.