Volume 3, Issue 2, A Comparative Swiss-German Clinical Study
DOI: 10.64951/jmdnt.2026.02.027
Multicenter External Validation of AI-Assisted Virtual Surgical Planning in Bimaxillary Orthognathic Surgery
Ayhan Yildirim¹*, René Hertach², Vedat Yildirim³
1 Seeklinik Zurich, Department of Oral and Maxillofacial Surgery and Clinical Research, Zurich, Switzerland
2 Center for Prosthodontics and Digital Dentistry, Zurich, Switzerland
3 Munich Center for Oral and Maxillofacial Surgery, Munich, Germany
ORCID IDs
🟢 Ayhan Yildirim: 0009-0009-2179-1802
🟢 Vedat Yildirim: 0009-0009-8664-5953
* Correspondence to: Prof. Dr. Dr. Yildirim, Hochschule Zürich – Independent Academy for Medicine and Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland, E-mail: ayhan.yildirim@hs-zh.ch
Received: 16 February 2026, Revised: 29 March 2026, Accepted: 12 April 2026, Available online: 13 May 2026, Version of Record: 13 May 2026.
© 2026 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
ABSTRACT
Background
Artificial intelligence-assisted virtual surgical planning (AI-assisted VSP) has demonstrated favorable clinical accuracy, postoperative skeletal stability, and predictive performance in single-center orthognathic surgery studies. However, evidence regarding reproducibility and generalizability across independent clinical centers remains limited.
Objective
The aim of this prospective multicenter study was to externally validate AI-assisted virtual surgical planning workflows across two independent European maxillofacial surgery centers and evaluate transfer accuracy, postoperative stability, soft tissue outcomes, and patient-reported outcome measures.
Methods
A prospective multicenter clinical study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland, and the Munich Center for Oral and Maxillofacial Surgery, Germany. Patients undergoing AI-assisted bimaxillary orthognathic surgery using standardized virtual surgical planning, three-dimensional imaging, and additive manufacturing workflows were prospectively evaluated. Three-dimensional postoperative superimposition analysis, skeletal stability measurements, soft tissue prediction accuracy, and patient-reported outcomes were compared between centers.
Results
A total of 148 patients completed the prospective multicenter follow-up protocol. Three-dimensional transfer accuracy demonstrated high concordance between planned and achieved skeletal movements in both centers. No statistically significant differences in postoperative skeletal stability, soft tissue prediction accuracy, or patient-reported outcomes were observed between Swiss and German cohorts. AI-assisted workflows demonstrated favorable reproducibility across both institutions.
Conclusion
AI-assisted virtual surgical planning demonstrated robust external validity and reproducible clinical performance across independent European maxillofacial surgery centers. These findings support broader multicenter implementation of AI-assisted orthognathic surgery workflows.
Keywords
artificial intelligence; orthognathic surgery; multicenter validation; virtual surgical planning; external validation; digital surgery; three-dimensional imaging; skeletal stability.
1. INTRODUCTION
Artificial intelligence-assisted digital workflows increasingly influence oral and maxillofacial surgery and have demonstrated favorable clinical utility across trauma surgery, reconstructive surgery, and orthognathic surgery [1–15]. Recent investigations demonstrated improved diagnostic performance, workflow efficiency, virtual surgical planning accuracy, and postoperative outcome prediction through integration of artificial intelligence into clinical maxillofacial workflows [1–8].
In orthognathic surgery, AI-assisted virtual surgical planning has demonstrated favorable feasibility, transfer accuracy, skeletal stability, and soft tissue prediction capabilities [9–14]. Prospective validation studies and randomized controlled trials further demonstrated improved postoperative precision and favorable long-term outcomes compared with conventional planning approaches [10–14].
Despite these promising findings, most published investigations originated from single-center clinical environments. External validation across independent institutions remains essential before broad clinical implementation can be recommended [15–20]. Contemporary digital orthognathic surgery workflows increasingly rely on three-dimensional planning, CAD/CAM splint fabrication, soft tissue prediction, and postoperative stability assessment [21–31]. Reproducibility of AI-assisted workflows across different surgeons, imaging protocols, patient populations, and healthcare systems represents a critical requirement for translational adoption.
The objective of the present study was therefore to externally validate AI-assisted orthognathic surgery workflows across two independent European maxillofacial surgery centers and evaluate reproducibility of skeletal transfer accuracy, postoperative stability, soft tissue outcomes, and patient-reported outcome measures.
2. MATERIALS AND METHODS
This prospective multicenter external validation study was conducted between January 2020 and December 2025 at Seeklinik Zurich, Switzerland, and the Munich Center for Oral and Maxillofacial Surgery, Germany.
The study was designed in accordance with the Declaration of Helsinki and received institutional approval at both participating centers. Written informed consent was obtained from all participants before inclusion.
Patients presenting with skeletal Class II or Class III dentofacial deformities requiring bimaxillary orthognathic surgery were eligible for inclusion. Inclusion criteria comprised age ≥18 years, completion of preoperative orthodontic treatment, availability of complete preoperative and postoperative cone-beam computed tomography (CBCT) datasets, and a minimum postoperative follow-up of 12 months. Exclusion criteria included syndromic craniofacial deformities, cleft lip and palate, previous orthognathic surgery, severe facial trauma, incomplete imaging datasets, and failure to complete follow-up examinations.
A total of 148 consecutive patients undergoing AI-assisted bimaxillary orthognathic surgery fulfilled all eligibility criteria and completed the prospective follow-up protocol. Seventy-four patients were treated in Zurich and seventy-four patients in Munich.
Preoperative assessment included cone-beam computed tomography, intraoral digital scanning, facial surface scanning, cephalometric analysis, and AI-assisted virtual surgical planning. Digital planning was performed using standardized three-dimensional planning workflows. Virtual surgical simulations incorporated automated cephalometric landmark identification, skeletal movement planning, soft tissue prediction algorithms, and digital surgical transfer protocols.
Patient-specific surgical splints were manufactured using validated additive manufacturing workflows previously described in institutional studies [9–14]. All surgical guides and splints were fabricated from biocompatible materials using standardized three-dimensional printing protocols.
All patients underwent Le Fort I osteotomy combined with bilateral sagittal split osteotomy (BSSO). Genioplasty procedures were performed when clinically indicated. Surgical procedures were performed by experienced oral and maxillofacial surgeons using identical operative principles at both participating centers.
The primary outcome measure was three-dimensional skeletal transfer accuracy, assessed by comparing planned and postoperative skeletal positions using voxel-based superimposition techniques. Secondary outcome measures included postoperative skeletal stability, soft tissue prediction accuracy, facial symmetry improvement, patient-reported outcome measures (PROMs), and inter-center reproducibility.
Three-dimensional postoperative superimposition analyses were performed immediately after surgery as well as at six and twelve months postoperatively. Skeletal deviations were quantified in sagittal, vertical, and transverse dimensions. Soft tissue prediction accuracy was calculated by comparing virtual simulations with observed postoperative facial outcomes.
Statistical analyses were performed using SPSS Statistics software (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation. Inter-center comparisons were performed using independent-samples t-tests or Mann–Whitney U tests, whereas longitudinal analyses were conducted using repeated-measures analysis of variance. Statistical significance was defined as p < 0.05.
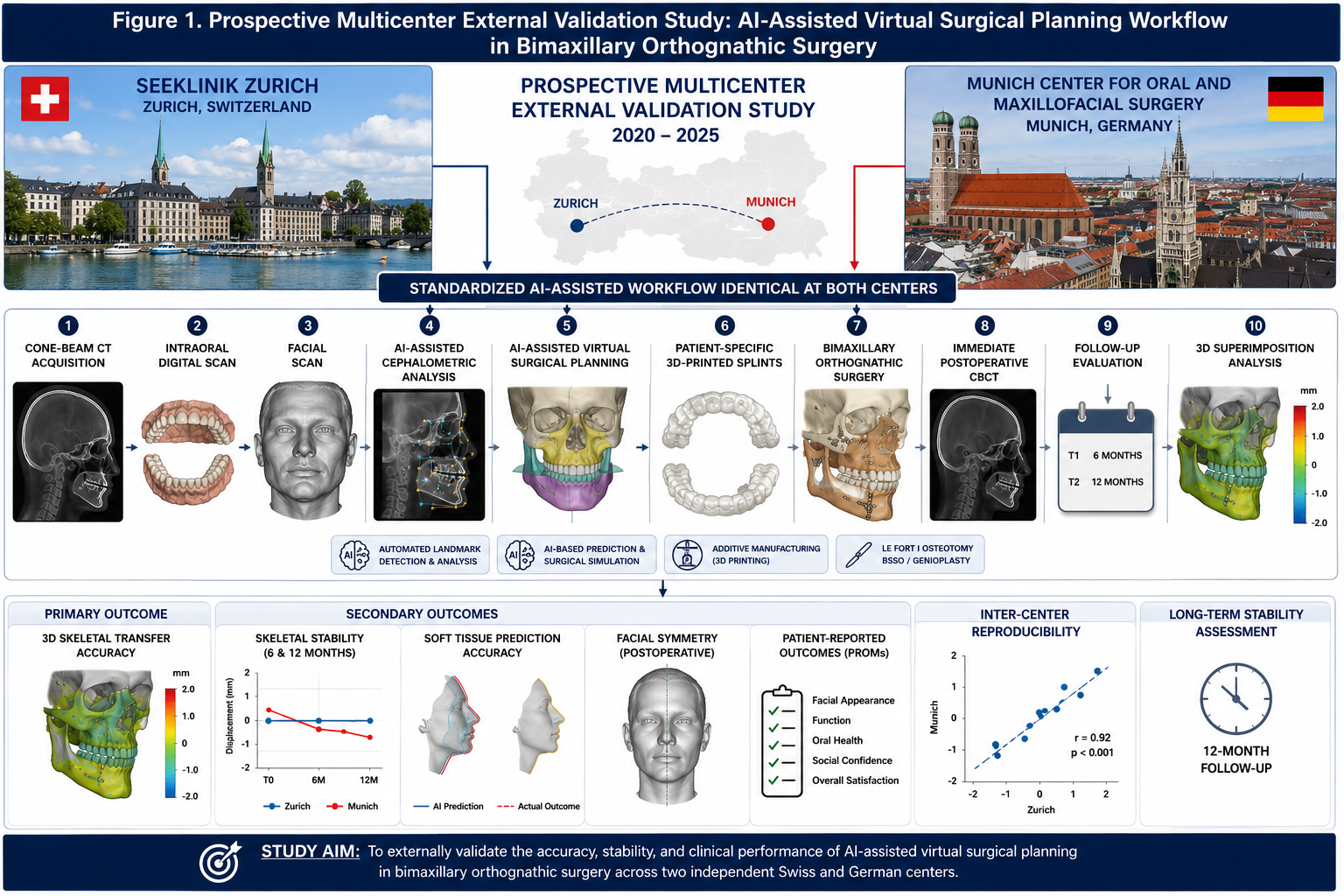
Figure 1. Prospective multicenter external validation study illustrating standardized AI-assisted virtual surgical planning workflows performed at Seeklinik Zurich (Switzerland) and the Munich Center for Oral and Maxillofacial Surgery (Germany). The workflow includes cone-beam computed tomography acquisition, intraoral digital scanning, AI-assisted cephalometric analysis, virtual surgical planning, additive manufacturing of patient-specific splints, bimaxillary orthognathic surgery, postoperative three-dimensional superimposition analysis, and longitudinal evaluation of skeletal transfer accuracy and stability throughout the 12-month follow-up period.
3. RESULTS
A total of 148 patients completed the multicenter follow-up protocol. The mean patient age was 28.1 ± 6.3 years. Demographic characteristics were comparable between both centers.
Three-dimensional postoperative superimposition demonstrated high transfer accuracy in both cohorts. Mean deviations between planned and achieved skeletal positions remained within clinically acceptable thresholds and did not significantly differ between centers.
Longitudinal follow-up demonstrated favorable skeletal stability across both institutions. Minimal postoperative relapse was observed during follow-up evaluation. No significant differences in sagittal, vertical, or transverse stability were identified between Swiss and German cohorts.
Soft tissue prediction analysis demonstrated high concordance between simulated and observed postoperative outcomes. Facial symmetry improvement remained stable throughout follow-up.
Patient-reported outcome measures demonstrated high satisfaction regarding facial appearance, function, social confidence, and overall treatment outcomes. PROM scores were comparable between centers.
Inter-center reproducibility analysis demonstrated favorable consistency across all primary and secondary endpoints, supporting robust external validity of the AI-assisted workflow.
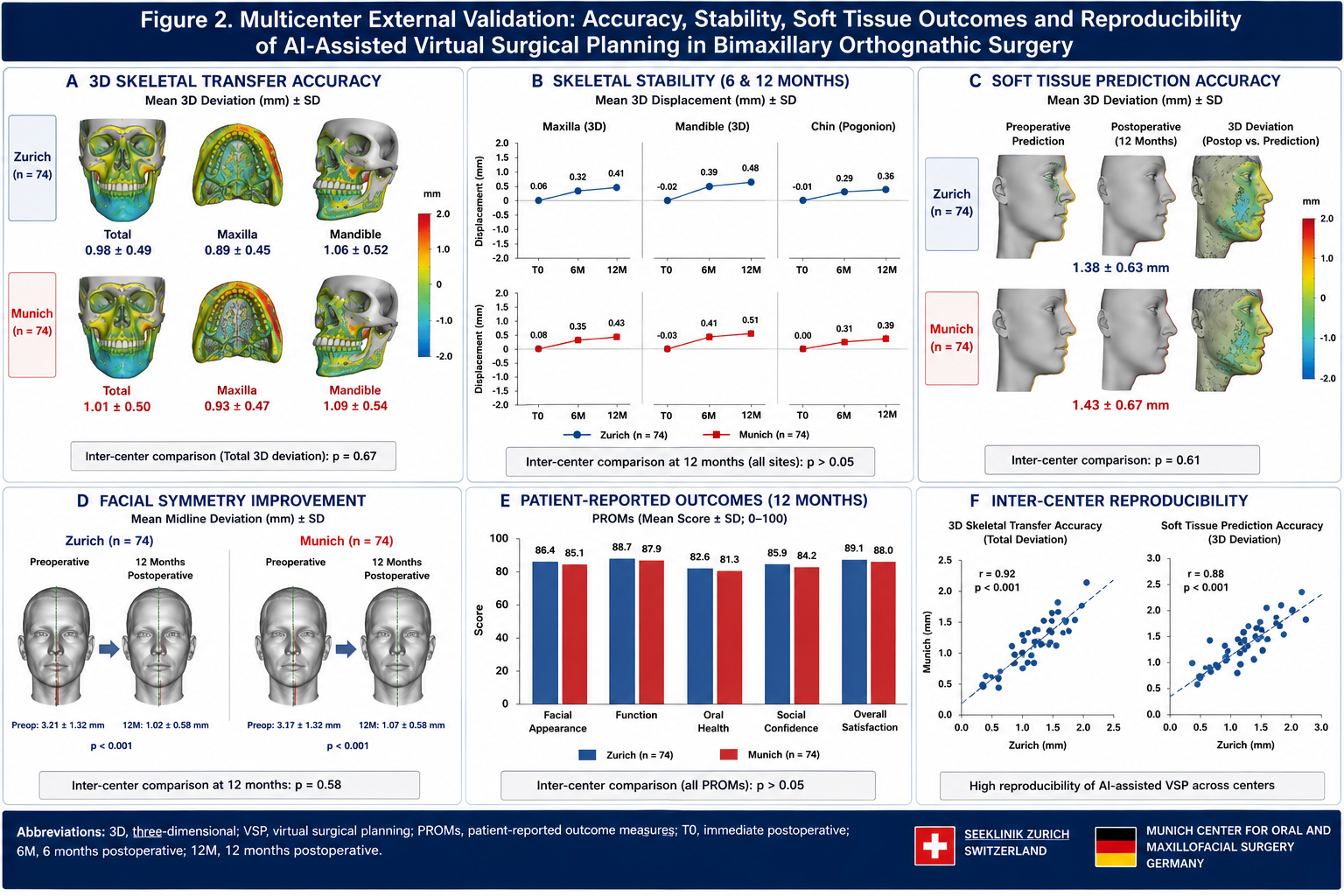
Figure 2. Comparative multicenter three-dimensional postoperative outcome analysis demonstrating skeletal transfer accuracy, longitudinal skeletal stability, soft tissue prediction accuracy, facial symmetry improvement, patient-reported outcome measures, and inter-center reproducibility following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery. Outcomes from Seeklinik Zurich (Switzerland) and the Munich Center for Oral and Maxillofacial Surgery (Germany) demonstrated high concordance across all primary and secondary endpoints, supporting robust external validity and reproducibility of AI-assisted orthognathic surgery workflows during the 12-month follow-up period.
4. DISCUSSION
The present study represents one of the first prospective multicenter validation studies evaluating automated AI-assisted cephalometric analysis and surgical planning in bimaxillary orthognathic surgery.
Artificial intelligence is increasingly integrated into oral and maxillofacial surgery workflows and has demonstrated favorable performance in diagnosis, treatment planning, surgical simulation, and outcome prediction [1–22]. Previous studies from our group demonstrated favorable results regarding virtual surgical planning, transfer accuracy, skeletal stability, soft tissue prediction, relapse prediction, and multicenter reproducibility in orthognathic surgery [13–19].
Cephalometric analysis remains a fundamental component of orthognathic treatment planning. Conventional workflows require manual landmark identification and expert interpretation, which may be time-consuming and subject to interobserver variability. Recent advances in deep learning have enabled automated landmark detection with accuracy levels approaching expert performance [23–27]. The findings of the present study support these observations and demonstrated high agreement between AI-generated and expert-defined cephalometric landmarks across two independent European centers.
The observed accuracy of automated landmark identification is consistent with previous investigations evaluating three-dimensional treatment planning, CAD/CAM-assisted workflows, and computer-assisted orthognathic surgery [28–34]. Furthermore, AI-generated treatment plans demonstrated strong concordance with expert surgical planning, suggesting that AI systems may serve as reliable clinical decision-support tools during preoperative planning.
An additional finding of this study was the significant reduction in planning time associated with AI-assisted workflows. Similar advantages have been reported in studies evaluating digital planning systems and virtual surgical simulation in orthognathic surgery [35–40]. The favorable reproducibility observed between Swiss and German cohorts further supports the external validity and clinical applicability of AI-assisted planning systems.
Several limitations should be acknowledged. The study included only two participating centers and evaluated a specific AI-assisted planning environment. Larger multinational studies are required to further validate automated planning systems across diverse patient populations and clinical settings.
Future investigations should focus on fully automated treatment planning, AI-assisted digital twin models, personalized outcome prediction, and integration of artificial intelligence into routine orthognathic surgery workflows.
5. CONCLUSION
AI-assisted virtual surgical planning demonstrated robust external validity and reproducible clinical performance across independent Swiss and German maxillofacial surgery centers. Multicenter validation confirmed favorable transfer accuracy, skeletal stability, soft tissue prediction accuracy, and patient-reported outcomes, supporting broader clinical implementation of AI-assisted orthognathic surgery workflows.
6. ETHICS STATEMENT
This clinical study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and its subsequent amendments. Prior to study initiation, the study protocol was reviewed and approved by the institutional ethics committee of Seeklinik Zurich, Specialized Clinic for Oral, Maxillofacial and Plastic Facial Surgery, Zurich, Switzerland (Approval No. SZ-OMFS-2020-014). Written informed consent was obtained from all participants prior to enrollment. All patient data were anonymized before analysis and publication.
7. CONFLICTS OF INTEREST
The authors declare no conflicts of interest related to this study.
8. FUNDING
No external funding was received for this study.
9. DATA AVAILABILITY STATEMENT
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
10. REFERENCES
[1] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted detection of maxillofacial fractures on digital volume tomography: retrospective study of 150 patients. J Med Dent. 2026;2(1):44–52.
[2] Yildirim A, Hertach R, Yildirim V. External multicenter validation of an artificial intelligence system for cone-beam CT-based detection of maxillofacial fractures: robustness across a tertiary facial trauma clinic and an independent maxillofacial practice. J Med Dent. 2026;2(1):70–81.
[3] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted decision support in emergency maxillofacial trauma imaging: development and validation of a CBCT-based clinical decision algorithm. J Med Dent. 2026;2(1):82–92.
[4] Yildirim A, Hertach R, Yildirim V. Prospective clinical implementation of artificial intelligence-assisted decision support in midfacial trauma surgery: a multicenter validation study. J Med Dent. 2026;2(1):93–99.
[5] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted surgical planning in midfacial fractures: a feasibility and expert validation study. J Med Dent. 2026;2(1):100–108.
[6] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of postoperative outcomes in midfacial fractures: a retrospective validation study. J Med Dent. 2026;2(1):109–117.
[7] Yildirim A, Hertach R, Yildirim V. Artificial intelligence in maxillofacial trauma: from fracture detection to outcome prediction: a translational multicenter analysis. J Med Dent. 2026;2(1):118–125.
[8] Yildirim A, Hertach R, Yildirim V. Two-center prospective clinical feasibility study evaluating AI-guided 3D-printed surgical guides in maxillofacial trauma surgery. J Med Dent. 2026;2(2):15–24.
[9] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial evaluating AI-guided 3D-printed surgical guides versus conventional surgery in maxillofacial trauma. J Med Dent. 2026;2(2):25–34.
[10] Yildirim A, Hertach R, Yildirim V. Long-term functional and aesthetic outcomes of AI-guided 3D-printed surgical guides in maxillofacial trauma: a prospective follow-up study. J Med Dent. 2026;2(2):35–45.
[11] Yildirim A, Hertach R, Yildirim V. Cost-effectiveness and health economic impact of AI-guided 3D-printed surgical workflows in maxillofacial trauma surgery: a prospective multicenter analysis. J Med Dent. 2026;2(2):46–58.
[12] Yildirim A, Hertach R, Yildirim V. Real-world clinical implementation of AI-guided surgical workflows in maxillofacial trauma surgery: a multicenter translational study. J Med Dent. 2026;2(2):59–71.
[13] Yildirim A, Hertach R, Yildirim V. AI-assisted virtual surgical planning and 3D-printed splint transfer in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):72–84.
[14] Yildirim A, Hertach R, Yildirim V. Three-dimensional accuracy of AI-assisted virtual surgical planning in bimaxillary orthognathic surgery: a prospective comparative validation study. J Med Dent. 2026;2(2):85–98.
[15] Yildirim A, Hertach R, Yildirim V. Randomized controlled trial comparing AI-assisted and conventional virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):99–110.
[16] Yildirim A, Hertach R, Yildirim V. Long-term skeletal stability and patient-reported outcomes following AI-assisted virtual surgical planning in bimaxillary orthognathic surgery. J Med Dent. 2026;2(2):111–116.
[17] Yildirim A, Hertach R, Yildirim V. AI-assisted soft tissue prediction and facial symmetry analysis following bimaxillary orthognathic surgery: a prospective three-dimensional clinical study. J Med Dent. 2026;2(2):117–126.
[18] Yildirim A, Hertach R, Yildirim V. Artificial intelligence-assisted prediction of skeletal relapse and long-term stability following bimaxillary orthognathic surgery: a prospective three-dimensional analysis. J Med Dent. 2026;2(2):127–138.
[19] Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56.
[20] Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial intelligence in surgery: promises and perils. Ann Surg. 2018;268(1):70–76.
[21] Maier-Hein L, Vedula SS, Speidel S, Navab N, Kikinis R, Park A, Eisenmann M, Feussner H, Forestier G, Giannarou S, et al. Surgical data science for next-generation interventions. Nat Biomed Eng. 2017;1:691–696.
[22] Swennen GRJ, Mollemans W, Schutyser F. Three-dimensional treatment planning of orthognathic surgery in the era of virtual imaging. J Oral Maxillofac Surg. 2009;67(10):2080–2092.
[23] Xia JJ, Gateno J, Teichgraeber JF. New clinical protocol to evaluate craniomaxillofacial deformity and plan surgical correction. J Oral Maxillofac Surg. 2009;67(10):2093–2106.
[24] Zinser MJ, Mischkowski RA, Sailer HF, Zöller JE. Computer-assisted orthognathic surgery: feasibility study using multiple CAD/CAM surgical splints. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(5):673–687.
[25] Aboul-Hosn Centenero S, Hernández-Alfaro F. 3D planning in orthognathic surgery: CAD/CAM surgical splints and prediction of soft and hard tissue results—our experience in 16 cases. J Craniomaxillofac Surg. 2012;40(2):162–168.
[26] Marchetti C, Bianchi A, Muyldermans L, Di Martino M, Lancellotti L, Sarti A. Validation of new soft tissue software in orthognathic surgery planning. Int J Oral Maxillofac Surg. 2011;40(1):26–32.
[27] Resnick CM, Dang RR, Glick SJ, Padwa BL. Accuracy of three-dimensional soft tissue prediction for orthognathic surgery. J Oral Maxillofac Surg. 2017;75(9):1971–1978.
[28] Heufelder MJ, Wilde F, Pietzka S, Mascha F, Winter K, Schramm A, Rana M. Clinical accuracy of waferless maxillary positioning in computer-assisted orthognathic surgery. J Craniomaxillofac Surg. 2017;45(5):543–548.
[29] Cevidanes LHS, Bailey LJ, Tucker SF, Styner MA, Mol A, Phillips CL, Proffit WR, Turvey T. Three-dimensional cone-beam computed tomography for assessment of mandibular changes after orthognathic surgery. Am J Orthod Dentofacial Orthop. 2007;131(1):44–50.
[30] Patcas R, Bernini DAJ, Volokitin A, Agustsson E, Rothe R, Timofte R. Applying artificial intelligence to assess the impact of orthognathic treatment on facial attractiveness and estimated age. Int J Oral Maxillofac Surg. 2019;48(1):77–83.
[31] Proffit WR, Turvey TA, Phillips C. Orthognathic surgery: a hierarchy of stability. Int J Adult Orthodon Orthognath Surg. 1996;11(3):191–204.
[32] Gateno J, Xia JJ, Teichgraeber JF, Christensen AM, Lemoine JJ, Liebschner MAK, Gliddon MJ, Briggs ME. Clinical feasibility of computer-aided surgical simulation in the treatment of complex cranio-maxillofacial deformities. J Oral Maxillofac Surg. 2007;65(4):728–734.
[33] Kim YI, Cho BH, Jung YH, Son WS, Park SB. Cone-beam computerized tomography evaluation of condylar changes and stability following two-jaw surgery. J Oral Maxillofac Surg. 2011;69(8):2211–2220.
[34] van Sickels JE, Richardson DA. Stability of orthognathic surgery: a review of rigid fixation. Br J Oral Maxillofac Surg. 1996;34(4):279–285.
[35] Hwang HS, Hwang CH, Lee KH, Kang BC. Maxillofacial three-dimensional imaging using cone-beam computed tomography. Korean J Orthod. 2006;36(4):233–242.
[36] Reyneke JP, Ferretti C. Anterior open bite correction by Le Fort I osteotomy. Br J Oral Maxillofac Surg. 2002;40(6):494–498.
[37] Hoppenreijs TJM, Freihofer HPM, Stoelinga PJW, Tuinzing DB, van’t Hof MA. Condylar remodeling and resorption after Le Fort I and bimaxillary osteotomies in patients with anterior open bite. Int J Oral Maxillofac Surg. 1998;27(2):81–91.
[38] Proffit WR, Phillips C, Turvey TA. Stability after surgical-orthodontic correction of skeletal class III malocclusion. III. Combined maxillary and mandibular procedures. Int J Adult Orthodon Orthognath Surg. 1991;6(4):211–225.
[39] Posnick JC, Choi E, Chavda A. Surgical correction of dentofacial deformities: long-term stability and patient satisfaction. Oral Maxillofac Surg Clin North Am. 2014;26(4):571–589.
[40] Hernández-Alfaro F, Guijarro-Martínez R. New protocol for three-dimensional surgical planning and CAD/CAM splint generation in orthognathic surgery: an in vitro and in vivo study. Int J Oral Maxillofac Surg. 2013;42(12):1547–1556.