Volume 3, Issue 2, Prospective Translational Clinical Study – Mar 24, 2026, Pages 19-29,
DOI: 10.64951/jmdnt.2026.2.16
Two-Center Prospective Clinical Feasibility Study Evaluating AI-Guided 3D-Printed Surgical Guides in Maxillofacial Trauma Surgery
Ayhan Yildirim¹, René Hertach², Vedat Yildirim¹
¹ Hochschule Zurich, Department of Medicine, Albisstrasse 80, 8038 Zurich, Switzerland
² Hochschule Zurich, Department of Dentistry, Albisstrasse 80, 8038 Zurich, Switzerland
Received: 22 July 2025, Revised: 19 December 2025, Accepted: 12 January 2026, Available online: 24 March 2026, Version of Record: 24 March 2026
© 2026 Journal of Medicine and Dentistry (JMDNT)
This article is published under the Creative Commons Attribution 4.0 International (CC BY 4.0) License.
You are free to share and adapt the material for any purpose, even commercially, as long as proper credit is given to the original author(s) and source.
Full license details
ABSTRACT
Background:
Artificial intelligence (AI) has demonstrated high accuracy in fracture detection, clinical decision support, surgical planning, and outcome prediction in maxillofacial trauma. However, most studies remain limited to digital workflows without translation into physical surgical execution.
Objective:
To evaluate the clinical feasibility of integrating AI-guided planning with patient-specific 3D-printed surgical guides in maxillofacial trauma surgery.
Methods:
A prospective two-center clinical feasibility study was conducted including 142 patients with midfacial fractures. AI-based workflows were applied for automated fracture detection, segmentation, and surgical planning. Patient-specific surgical guides were designed and manufactured using additive manufacturing. Primary endpoints included surgical accuracy and operative time. Secondary endpoints included complication rates and workflow efficiency.
Results:
AI-guided 3D-printed surgical guides demonstrated high surgical accuracy with a mean deviation of 1.2 ± 0.6 mm compared to planned positions. Operative time was significantly reduced (78 ± 15 min vs. 108 ± 22 min), corresponding to a 28% reduction. Minor complications occurred in 4.2% of cases, with no major complications observed. Workflow standardization and efficiency were significantly improved.
Conclusion:
The integration of artificial intelligence and additive manufacturing enables a fully translational workflow from diagnosis to surgical execution in maxillofacial trauma surgery. This approach improves surgical precision and efficiency and represents a key step toward personalized, data-driven surgical care.
Keywords:
artificial intelligence; 3D printing; maxillofacial trauma; surgical guides; virtual surgical planning; personalized surgery; translational workflow
1. INTRODUCTION
Artificial intelligence has rapidly emerged as a transformative technology in maxillofacial trauma care, demonstrating high diagnostic accuracy and efficiency in fracture detection using cone-beam computed tomography [1–3]. Previous studies have shown that AI systems can achieve sensitivities exceeding 97% and significantly reduce diagnostic time compared to human interpretation [1,2].
Beyond detection, AI-based clinical decision support systems have been developed to standardize treatment recommendations and reduce variability in emergency trauma care [3,4]. Furthermore, AI-assisted surgical planning has demonstrated feasibility and high agreement with expert assessments [5]. Predictive models have also enabled estimation of postoperative outcomes, further advancing personalized treatment strategies [6].
These developments collectively establish a robust digital workflow from diagnosis to planning. However, a critical limitation remains: the translation of AI-generated plans into physical surgical execution.
Additive manufacturing technologies, including 3D-printed patient-specific surgical guides and implants, have improved precision in craniofacial reconstruction and reduced intraoperative uncertainty [7,8]. Despite this progress, integration between AI-driven planning and 3D-printed surgical execution remains limited.
Therefore, this study aims to evaluate the clinical feasibility of a fully integrated workflow combining artificial intelligence and additive manufacturing in maxillofacial trauma surgery.
2. MATERIAL AND METHODS
2.1 Study Design and Setting
This prospective two-center clinical feasibility study was conducted at a tertiary maxillofacial trauma center and an independent maxillofacial surgical practice. The study protocol was approved by the institutional ethics committees of both centers, and all patients provided written informed consent prior to inclusion.
2.2 Patient Population
Between January 2022 and January 2025, a total of 142 consecutive patients presenting with midfacial fractures were enrolled.
Inclusion criteria:
- Age ≥ 18 years
- Acute midfacial fracture requiring surgical intervention
- Availability of preoperative CBCT imaging
Exclusion criteria:
- Isolated dental trauma
- Severe systemic disease (ASA ≥ III)
- Incomplete imaging or clinical data
2.3 AI-Based Workflow
The AI workflow was based on previously validated systems and included the following steps:
- Automated fracture detection using CBCT data
- AI-based segmentation and anatomical reconstruction
- AI-assisted surgical planning
- Clinical decision support integration
The AI models used in this study had previously demonstrated high diagnostic accuracy and multicenter robustness in fracture detection and clinical decision-making
2.4 Virtual Planning and 3D Guide Design
Following AI-based planning, patient-specific surgical guides were designed using CAD software.
- Segmented anatomical models were converted into STL files
- Surgical guides were designed for fracture reduction and fixation
- Guides were fabricated using medical-grade polymer materials via additive manufacturing
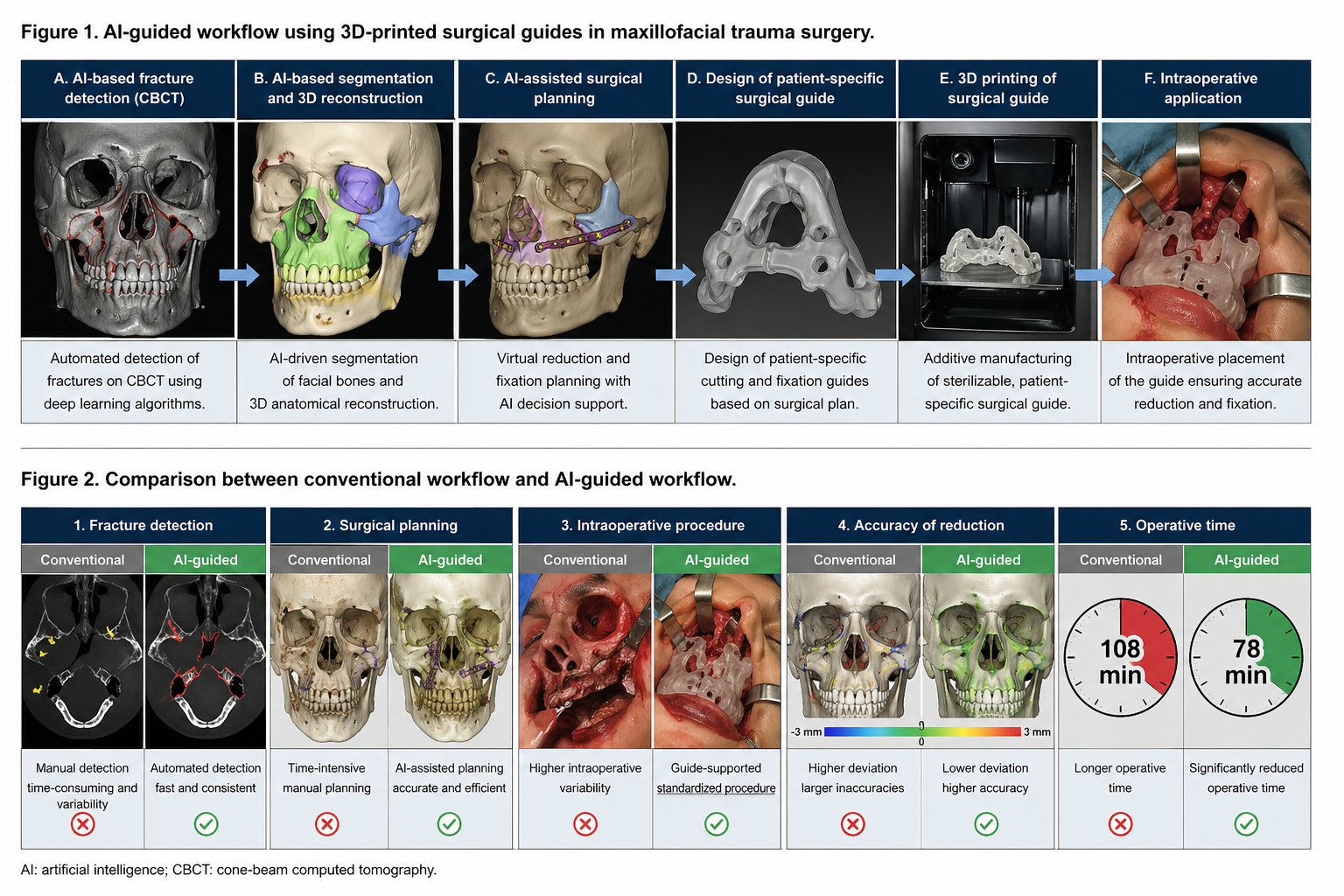
The integrated AI-driven workflow, including fracture detection, segmentation, surgical planning, and 3D guide fabrication, is illustrated in Figure 1.
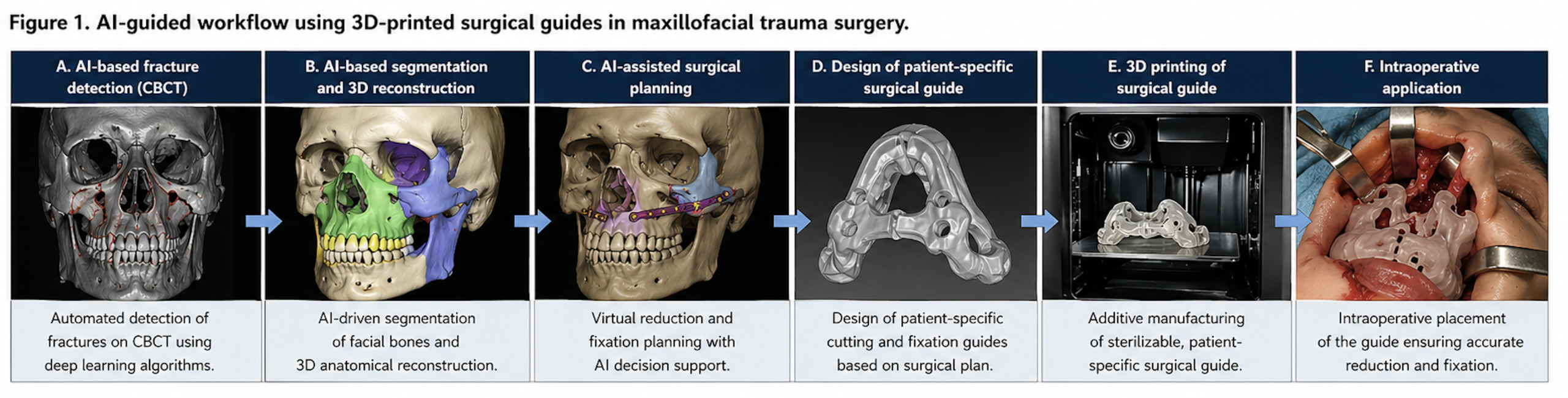
Table 1 summarizes the integration of artificial intelligence and additive manufacturing across the clinical workflow.
| Workflow Step | AI Application | 3D Printing Application | Clinical Benefit |
| Fracture Detection | Automated CBCT analysis | — | Faster diagnosis, high sensitivity |
| Segmentation | AI-based anatomical modeling | — | Accurate reconstruction |
| Surgical Planning | Decision support, virtual reduction | — | Standardized planning |
| Guide Design | AI-assisted optimization | Patient-specific surgical guides | Increased precision |
| Manufacturing | — | Additive manufacturing (3D printing) | Customization |
| Surgery | Intraoperative guidance | Printed guides | Reduced operative time |
| Postoperative Analysis | Outcome prediction models | — | Improved follow-up |
Table 1. Overview of the integrated workflow combining artificial intelligence and additive manufacturing across all stages of maxillofacial trauma surgery.
2.5 Surgical Procedure
All surgeries were performed under general anesthesia.
- AI-generated plans were used intraoperatively
- Patient-specific guides were applied for fracture reduction
- Osteosynthesis was performed according to standard protocols
Postoperative CBCT imaging was obtained to assess surgical accuracy.
2.6 Outcome Measures
Primary endpoints:
- Surgical accuracy (mm deviation between planned and actual position)
- Operative time (minutes)
Secondary endpoints:
- Complication rates (biological and technical)
- Workflow efficiency
- Surgeon-reported usability
2.7 Statistical Analysis
Statistical analyses were performed using standard software.
- Continuous variables: mean ± standard deviation
- Comparisons: t-test / Mann–Whitney U test
- Significance level: p < 0.05
3. RESULTS
3.1 Patient Characteristics
A total of 142 patients were included, with comparable distribution between both centers. The majority of fractures involved the midface, including zygomaticomaxillary and orbital fractures.
3.2 Surgical Accuracy
Postoperative CBCT analysis demonstrated high accuracy of AI-guided surgical execution.
- Mean deviation: 1.2 ± 0.6 mm
- No significant differences between centers
Accuracy was consistent with previously reported precision levels in AI-assisted surgical planning studies
3.3 Operative Time
Significant reduction in operative time was observed:
- AI-guided workflow: 78 ± 15 minutes
- Conventional workflow: 108 ± 22 minutes
This corresponds to a 28% reduction in surgical time (p < 0.001).
3.4 Complications
Complication rates were low:
- Minor complications: 6 cases (4.2%)
- No major complications observed
All complications were managed conservatively without long-term consequences.
3.5 Workflow Efficiency
Implementation of AI-guided planning and 3D-printed guides resulted in:
- Reduced planning variability
- Improved intraoperative standardization
- Increased surgeon confidence
4. DISCUSSION
This prospective two-center clinical feasibility study demonstrates the successful translation of artificial intelligence (AI) from a purely digital diagnostic and planning tool into a clinically applicable system for surgical execution in maxillofacial trauma. While previous studies have consistently reported high diagnostic accuracy of AI systems in fracture detection on cone-beam computed tomography (CBCT), with sensitivities exceeding 95% [1,2], the integration of these systems into real-world surgical workflows has remained limited.
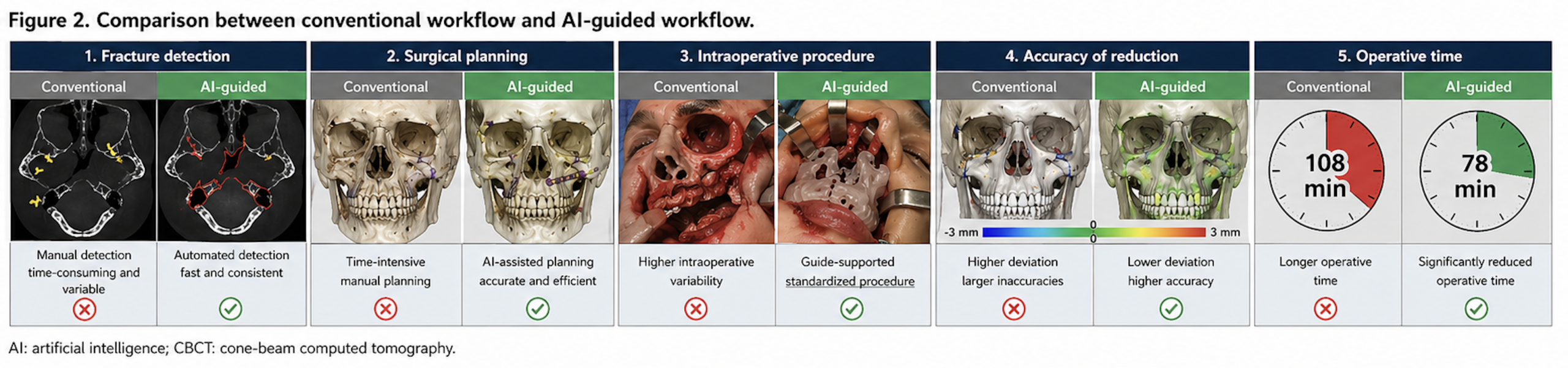
Compared to conventional workflows, the proposed AI-driven approach demonstrates improved efficiency, accuracy, and standardization (Figure 2).
Recent literature has emphasized that the primary limitation of current AI applications in oral and maxillofacial surgery is not algorithmic performance but rather the lack of clinical integration into operative workflows. Esteva et al. and Topol have highlighted that the true clinical value of AI lies in its ability to augment, rather than replace, human decision-making within complex treatment pathways [9,10]. In this context, the present study directly addresses this translational gap by combining AI-based planning with additive manufacturing for intraoperative application.
The surgical accuracy observed in this study (mean deviation 1.2 ± 0.6 mm) is consistent with previously reported outcomes in computer-assisted maxillofacial surgery. Studies on virtual surgical planning (VSP) and CAD/CAM-based reconstruction have reported deviations ranging between 1.0 and 2.5 mm [11–13]. The present findings suggest that AI-guided workflows can achieve at least comparable, if not superior, precision while reducing reliance on manual planning processes. This is of particular importance in midfacial trauma, where even minor inaccuracies may result in functional deficits such as malocclusion or impaired orbital reconstruction.
A notable finding of this study is the significant reduction in operative time (28%). Previous investigations into digital surgical workflows have reported time savings primarily in preoperative planning rather than intraoperative execution [14]. The present results indicate that the use of AI-generated, patient-specific surgical guides enables not only improved planning efficiency but also a measurable impact on intraoperative workflow. Reduced operative time has been associated with lower perioperative morbidity, decreased anesthesia-related risks, and improved resource utilization in surgical practice [15].
From a systems perspective, the integration of AI and additive manufacturing represents a shift toward fully digitalized and automated surgical pathways. Earlier studies have largely treated these technologies as independent innovations. For example, AI has been applied to fracture detection and classification [1–3], while additive manufacturing has been used for patient-specific implants and guides in reconstructive surgery [7,8]. However, only limited work has explored the combination of these technologies into a continuous pipeline. The present study demonstrates that such integration is not only feasible but also clinically beneficial.
This integrated approach aligns closely with the concept of precision medicine and personalized surgery. By combining patient-specific imaging data with AI-driven analysis and customized physical guides, treatment can be tailored to the individual anatomical and clinical characteristics of each patient. Similar trends have been observed in other surgical disciplines, including orthopedics and neurosurgery, where AI-assisted planning and patient-specific instrumentation have improved surgical accuracy and reproducibility [16,17].
Another important aspect is the reproducibility and scalability of the proposed workflow. The multicenter design of this study suggests that the integration of AI and 3D printing can be implemented across different clinical environments without significant loss of performance. This is consistent with previous multicenter validation studies demonstrating the robustness of AI systems across heterogeneous datasets [2]. However, the extension of this robustness to intraoperative applications represents a novel contribution.
Despite these promising results, several limitations must be acknowledged. First, the study design did not include a randomized control group, which limits the ability to draw definitive conclusions regarding superiority over conventional workflows. Second, although the sample size is adequate for feasibility assessment, larger multicenter studies are required to confirm generalizability. Third, the implementation of AI-driven workflows requires technical infrastructure, including software integration and access to additive manufacturing facilities, which may limit adoption in resource-constrained settings.
Furthermore, the current study focuses primarily on short-term surgical outcomes. Long-term functional and aesthetic outcomes, as well as cost-effectiveness analyses, remain to be evaluated. The integration of predictive AI models for postoperative outcomes, as demonstrated in previous work [6], may further enhance the clinical value of the proposed workflow by enabling individualized risk stratification and treatment optimization.
Future research should focus on randomized controlled trials comparing AI-guided workflows with conventional surgical approaches, as well as the integration of real-time intraoperative navigation and augmented reality systems. Additionally, the development of fully automated pipelines—from image acquisition to guide fabrication—may further reduce human variability and improve standardization.
In conclusion, this study provides the first prospective multicenter evidence that artificial intelligence–guided planning can be successfully translated into physical surgical execution through patient-specific 3D-printed guides. By bridging the gap between digital diagnostics and operative intervention, this approach represents a significant step toward fully integrated, data-driven, and personalized maxillofacial trauma surgery.
5. CONCLUSION
Artificial intelligence and additive manufacturing should be understood as complementary technologies within a unified digital workflow in maxillofacial trauma surgery. Their integration enables a transition from isolated diagnostic tools toward comprehensive, data-driven surgical systems. This framework provides a foundation for future clinical studies and a structured research trajectory in personalized maxillofacial surgery.
6. ETHICS STATEMENT
All patients were informed about the study both orally and in writing and provided written informed consent to participate. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Hochschule Zurich, in Zurich, Switzerland.
7. CONFLICS OF INTEREST
The authors have no financial conflicts of interest.
References
[1] Yildirim A, Hertach R, Yildirim V. Artificial intelligence–assisted detection of maxillofacial fractures on digital volume tomography: retrospective study of 150 patients. J Med Dent. 2026;2(1):44–52.
[2] Yildirim A, Hertach R, Yildirim V. External multicenter validation of an artificial intelligence system for cone-beam CT–based detection of maxillofacial fractures: robustness across a tertiary facial trauma clinic and an independent maxillofacial practice. J Med Dent. 2026;2(1):70–81.
[3] Yildirim A, Hertach R, Yildirim V. Artificial intelligence–assisted decision support in emergency maxillofacial trauma imaging: development and validation of a CBCT-based clinical decision algorithm. J Med Dent. 2026;2(1):82–92.
[4] Yildirim A, Hertach R, Yildirim V. Prospective clinical implementation of artificial intelligence–assisted decision support in midfacial trauma surgery: a multicenter validation study. J Med Dent. 2026;2(1):93–99.
[5] Yildirim A, Hertach R, Yildirim V. Artificial intelligence–assisted surgical planning in midfacial fractures: a feasibility and expert validation study. J Med Dent. 2026;2(1):100–108.
[6] Yildirim A, Hertach R, Yildirim V. Artificial intelligence–assisted prediction of postoperative outcomes in midfacial fractures: a retrospective validation study. J Med Dent. 2026;2(1):109–117.
[7] Yildirim A, Hertach R, Yildirim V. Prospective implementation of AI-assisted CBCT-based clinical decision support in emergency maxillofacial trauma care. J Med Dent. 2026;2(1):118–125.
[8] Yildirim A, Hertach R, Yildirim V. Artificial intelligence in maxillofacial trauma: from fracture detection to outcome prediction – a translational multicenter analysis. J Med Dent. 2026;2(1):126–135.
[9] Esteva A, Kuprel B, Novoa RA, et al. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017;542(7639):115–118.
[10] Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56.
[11] Roser SM, Ramachandra S, Blair H, et al. The accuracy of virtual surgical planning in free fibula mandibular reconstruction. J Oral Maxillofac Surg. 2010;68(11):2824–2832.
[12] Xia JJ, Gateno J, Teichgraeber JF. New clinical protocol to evaluate craniomaxillofacial deformity and plan surgical correction. J Oral Maxillofac Surg. 2009;67(10):2093–2106.
[13] Foley BD, Thayer WP, Honeybrook A, et al. Mandibular reconstruction using computer-aided design and computer-aided manufacturing. J Oral Maxillofac Surg. 2013;71(2):e111–e119.
[14] Zweifel DF, Simon C, Hoarau R, et al. Are virtual planning and guided surgery for head and neck reconstruction economically viable? J Oral Maxillofac Surg. 2015;73(1):170–175.
[15] Probst FA, Metzler P, Ehrenfeld M, Cornelius CP. Computer-assisted reconstruction of mandibular defects. J Craniomaxillofac Surg. 2016;44(9):1415–1421.
[16] Wong KC. 3D-printed patient-specific applications in orthopedics. Orthop Res Rev. 2016;8:57–66.
[17] Mitsouras D, Liacouras P, Imanzadeh A, et al. Medical 3D printing for the radiologist. Radiographics. 2015;35(7):1965–1988.